

Chiropractor Services
Chiropractic Rehabilitation & Neuro-Structural Care: A Comprehensive Guide for Colorado Injury Patients

Chiropractic rehabilitation, also known as neuro-musculoskeletal medicine, is a healthcare discipline focused on diagnosing and treating mechanical disorders of the spine and nervous system—particularly injuries resulting from trauma such as motor vehicle collisions. Unlike emergency medicine (which addresses life-threatening injuries), chiropractic care specializes in identifying and correcting soft tissue damage, ligament laxity, and structural misalignments that often go undetected in traditional hospital settings.
This distinction matters profoundly for accident victims. While emergency departments excel at ruling out fractures, hemorrhaging, and organ damage, they are not equipped to assess the subtle—but devastating—biomechanical changes that occur during high-velocity impacts. These “invisible” injuries often manifest weeks or months after the initial trauma, creating chronic pain syndromes that could have been prevented with proper early intervention.
Connect with Specialized Auto Injury Providers
If you’ve been injured in a motor vehicle collision, connecting with a chiropractor who specializes in trauma documentation and insurance coordination is critical to both your recovery and your legal rights. Understanding the treatment options available can help you make informed decisions about your care.
Table of Contents[Hide][Show]
- Understanding the Biomechanics of Spinal Trauma
- The Diagnostic Gap: What Emergency Rooms Miss
- Core Treatment Modalities in Modern Chiropractic Care
- Advanced Diagnostic Technologies in Spinal Assessment
- The Neuro-Structural Approach to Injury Recovery
- The Recovery Timeline: What to Expect from Initial Injury to Stabilization
- When to Seek Chiropractic Care vs. Other Specialists

Explore Treatment Protocols by Injury Type:

Car Accident Treatments
Car Accident & Trauma Treatment Protocols
— Comprehensive acute injury management and rehabilitation

Spinal Decompression Therapy
Non-Surgical Spinal Decompression Therapy
— Advanced disc herniation and nerve compression treatment

Laser Therapy
Cold Laser Therapy for Inflammation & Healing
— Photobiomodulation for tissue repair and pain reduction

Percussor Therapy
Percussor Therapy for Deep Tissue Rehabilitation
— Mechanical soft tissue mobilization for scar tissue and adhesions
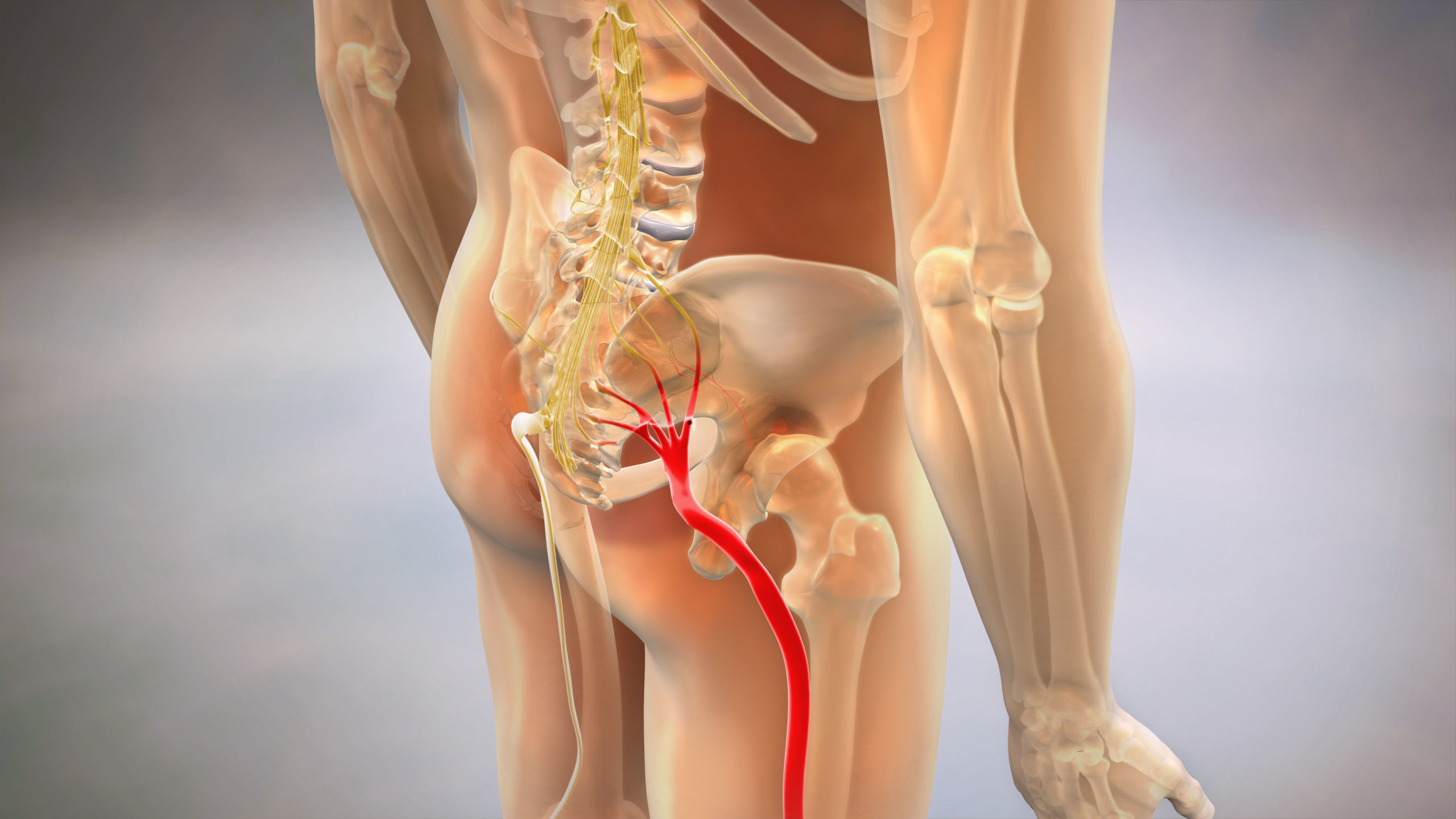
Sciatica Pain Relief
Sciatica & Nerve Pain Relief Treatments
— Targeted interventions for radiating pain and nerve irritation

Chiropractic Adjustments
Chiropractic Adjustments & Spinal Correction
— Structural realignment and joint mobilization techniques
Connecting with the right specialist matters. Our featured providers are credentialed in auto injury rehabilitation, advanced diagnostics (DMX/MRI), and insurance documentation protocols specific to Colorado motor vehicle claims.
Find a Featured Provider Near You
All featured providers accept Med-Pay and Attorney Lien arrangements
Understanding the Biomechanics of Spinal Trauma

The human spine is engineered to withstand substantial compressive forces during normal daily activities—lifting, bending, twisting. What it is not designed to handle is the rapid acceleration-deceleration that occurs during vehicular collisions, even at relatively low speeds.
Cervical Acceleration-Deceleration (CAD), commonly known as whiplash, involves a complex sequence of events that occur in milliseconds. During rear-end impact, the torso is thrust forward while the head remains momentarily stationary due to inertia. This creates a “S-curve” deformation of the cervical spine that exceeds normal physiological ranges of motion. The skull then snaps backward (hyperextension) before rebounding forward (hyperflexion).
This violent motion stretches and tears the ligaments, tendons, and muscle fibers that stabilize the neck. More critically, it can cause ligament laxity—permanent lengthening of the connective tissue that holds vertebrae in proper alignment. Unlike muscle strains that heal in weeks, ligamentous injuries can create chronic instability that persists for years.
The force vectors involved explain why symptoms often seem disproportionate to visible vehicle damage. A 15 mph collision can generate 5-7 G-forces on the cervical spine—equivalent to a force of 35-50 pounds applied to the head. This biomechanical reality is why “minor” accidents frequently produce major injuries.
The secondary phase of injury involves neuro-inflammation. When spinal tissues are damaged, the body’s immune system floods the area with inflammatory cytokines. While this is part of the healing process, chronic inflammation can sensitize nerve endings, creating a pain amplification cycle that transforms acute injury into chronic pain syndrome.
The Diagnostic Gap: What Emergency Rooms Miss
Emergency departments serve a critical function: ruling out life-threatening conditions. Their protocols are designed to identify fractures, internal bleeding, and neurological emergencies requiring immediate surgical intervention. They excel at this mission.
What they systematically miss are the soft tissue injuries that define most collision trauma. Standard emergency imaging—basic X-rays and CT scans—cannot visualize ligament tears, muscle strains, or disc bulges. An MRI can detect these pathologies, but emergency protocols rarely include MRI unless there are “red flag” symptoms like loss of bowel control or progressive paralysis.
The result is a dangerous gap in care. A patient leaves the ER with a diagnosis of “neck strain” and instructions to take ibuprofen, while underneath the surface, significant structural damage is unfolding. By the time symptoms become unbearable weeks later, scar tissue has formed, inflammation has become chronic, and the window for optimal intervention has closed.
Chiropractic physicians who specialize in trauma care fill this diagnostic void using functional assessment tools. Digital Motion X-Ray (DMX), for example, captures the spine during movement, revealing instabilities that static imaging misses entirely. Surface electromyography (sEMG) measures muscle guarding patterns—the body’s protective response to underlying joint dysfunction.
This is not a criticism of emergency medicine; it is an acknowledgment of scope of practice. Emergency physicians are not trained in biomechanical assessment because it falls outside their clinical mandate. Chiropractors specializing in neuro-structural rehabilitation are specifically educated to identify and correct these mechanical disorders.
The clinical implication for accident victims is clear: an emergency clearance is necessary but not sufficient. Comprehensive evaluation by a provider trained in functional biomechanics should be considered standard post-collision care, not an optional “add-on.”
Core Treatment Modalities in Modern Chiropractic Care
Contemporary chiropractic rehabilitation for trauma patients involves a multi-modal approach tailored to the phase and severity of injury.
Acute Phase (Days 0-14): The primary goals are inflammation control, pain reduction, and preventing the formation of pathological scar tissue. Gentle mobilization techniques restore limited range of motion without aggravating injured tissues. Cold laser therapy (Class IV photobiomodulation) penetrates deep tissue layers to reduce pro-inflammatory markers at the cellular level. Cryotherapy and electrical stimulation modulate pain signals while promoting lymphatic drainage.
Sub-Acute Phase (Weeks 2-8): As acute inflammation subsides, treatment shifts toward restoring proper joint mechanics and addressing compensatory patterns. Specific spinal adjustments using Gonstead, Diversified, or instrument-assisted techniques correct vertebral subluxations—misalignments that restrict motion and irritate nerve roots. Myofascial release and trigger point therapy address the muscle guarding patterns that developed during the acute phase.
Corrective/Rehabilitative Phase (Weeks 8-24): The focus becomes structural stability and preventing recurrence. Spinal decompression therapy—using traction-based devices or inversion protocols—reduces intradiscal pressure and promotes hydration of damaged discs. Therapeutic exercise prescriptions strengthen the deep cervical flexors and core stabilizers that protect against future injury. Postural retraining corrects the forward head posture and thoracic kyphosis that commonly develop after whiplash.
Maintenance Phase (Long-Term): For patients with residual ligament laxity or degenerative changes, periodic maintenance care prevents symptom flare-ups and slows the progression of post-traumatic arthritis.
The sophistication of modern techniques stands in stark contrast to outdated stereotypes of chiropractic care. Today’s trauma-focused practitioners integrate evidence-based protocols from sports medicine, neurology, and orthopedics—creating a truly integrative approach to neuro-musculoskeletal rehabilitation.
Advanced Diagnostic Technologies in Spinal Assessment
Accurate diagnosis precedes effective treatment. The diagnostic technologies employed by advanced chiropractic practices provide insights that traditional imaging often misses.
Digital Motion X-Ray (DMX) represents a quantum leap in functional assessment. Unlike static X-rays that capture a single position, DMX records video fluoroscopy as the patient moves through ranges of motion. This reveals ligamentous instability, aberrant motion patterns, and segmental dysfunction that only appear during movement. For medico-legal purposes, DMX provides objective documentation of soft tissue injuries that would otherwise be classified as “subjective complaints.”
Surface Electromyography (sEMG) measures the electrical activity of paraspinal muscles. In a healthy spine, left and right muscle groups exhibit symmetrical activation patterns. After injury, protective muscle spasm creates asymmetry as the nervous system attempts to stabilize damaged segments. sEMG quantifies this dysfunction, providing both a diagnostic baseline and objective progress markers during rehabilitation.
Thermography uses infrared sensors to detect temperature variations along the spine. Because nerve irritation alters local blood flow, thermographic scans can identify areas of neurological dysfunction before they become symptomatic. This technology is particularly valuable for detecting autonomic nervous system involvement—a common but under-recognized consequence of upper cervical trauma.
Computerized Range-of-Motion (CROM) Testing precisely measures cervical and lumbar mobility in six planes of movement. Establishing baseline restrictions allows clinicians to track functional improvements quantitatively, moving beyond subjective “how do you feel?” assessments to objective outcome data.
The integration of these technologies transforms chiropractic assessment from an art into a science. For patients navigating insurance claims or litigation, this objective documentation can mean the difference between claim approval and denial.
The Neuro-Structural Approach to Injury Recovery

Traditional symptom-based care asks: “Where does it hurt?” Neuro-structural rehabilitation asks: “What is causing the pain, and how do we correct the underlying dysfunction?”
This philosophical distinction shapes treatment priorities. Conventional approaches may focus primarily on pain relief through medication, injections, or passive modalities. While these interventions have value in acute phases, they do not address the structural and neurological causes perpetuating the pain cycle.
The neuro-structural model recognizes that the spine functions as an integrated kinetic chain. When one segment is damaged, the entire system compensates. A whiplash injury to the upper cervical spine, for example, often triggers compensatory lumbar hypermobility as the body attempts to maintain balance. Treating the neck pain while ignoring the lumbar compensation guarantees incomplete recovery.
Central to this approach is the concept of neuroplasticity—the nervous system’s ability to reorganize itself. Chronic pain rewires neural pathways, creating a “pain memory” that persists even after tissues have healed. Effective rehabilitation must therefore address both the structural injury and the neurological dysfunction it created.
Specific adjustments restore proper motion to restricted joints, sending proprioceptive signals to the brain that override pain signals. Rehabilitation exercises retrain motor patterns, breaking the dysfunctional movement habits the body adopted to avoid pain. This integrated approach addresses the injury at multiple levels simultaneously: structural, neurological, and functional.
The outcome difference is measurable. Studies comparing passive symptom management to active neuro-structural rehabilitation consistently show superior long-term outcomes for patients receiving corrective care—including reduced pain intensity, improved function, and lower recurrence rates.
Navigating Insurance & Medical-Legal Documentation in Colorado
For car accident victims, the medical-legal landscape can be as bewildering as the injury itself. Understanding your insurance rights and the importance of proper documentation protects both your health and your financial recovery.
Colorado Med-Pay Coverage: Under Colorado Revised Statutes Title 10, Article 4, Part 7, all auto insurance policies issued in the state must include Medical Payments (Med-Pay) coverage unless explicitly rejected in writing. This coverage typically provides $5,000 to $10,000 for medical expenses resulting from auto accidents, regardless of fault. Critically, Med-Pay reimburses directly—you do not need to wait for a settlement to receive treatment.
Many accident victims are unaware of this coverage and delay care due to financial concerns. This delay worsens both clinical outcomes and claim valuations, as insurance adjusters interpret treatment gaps as evidence that injuries were “not that serious.”
Personal Injury Protection (PIP): While not mandatory in Colorado, PIP coverage (when elected) provides broader benefits than Med-Pay, including wage loss reimbursement and replacement services. Understanding the specific coverage limits and exclusions in your policy is essential for maximizing benefits.
Lien-Based Care: When Med-Pay is exhausted or when fault is disputed, many trauma-focused chiropractic practices accept attorney liens. This means treatment proceeds immediately, with payment deferred until settlement or judgment. The provider assumes financial risk, which is why thorough documentation becomes crucial—both parties need a successful claim outcome.
Documentation Standards: Insurance companies and opposing counsel scrutinize chiropractic records intensely. Proper documentation includes:
Providers experienced in medico-legal cases understand that their clinical notes may become evidence. Vague entries like “patient improved” hold no weight in litigation. Quantified outcomes—”cervical rotation improved from 45° to 70°”—establish causation and validate treatment necessity.
Connect with a Verified Auto Injury Specialist
Financial concerns should never delay necessary medical care. Our featured providers specialize in navigating Colorado insurance protocols and offer consultation to review your coverage options before treatment begins.
The Recovery Timeline: What to Expect from Initial Injury to Stabilization
Understanding the typical healing trajectory helps set realistic expectations and reduces the anxiety that often compounds physical pain.
Week 1-2 (Acute Inflammatory Phase): Pain is typically at its peak during this period, often worsening on days 2-3 post-injury as inflammation reaches maximum levels. Stiffness, headaches, and difficulty sleeping are common. Treatment focuses on inflammation control and gentle mobilization. Patients should avoid prolonged sitting and use ice therapy (15 minutes per hour during waking hours).
Week 3-6 (Proliferative Phase): The body begins laying down collagen fibers to repair torn tissues. This is when scar tissue formation can become problematic if mobility is not maintained. Treatment intensifies to include specific adjustments and soft tissue work to guide proper healing alignment. Many patients experience significant symptom relief during this phase, but discontinuing care prematurely risks incomplete healing.
Week 7-12 (Remodeling Phase): Scar tissue matures and tissues regain tensile strength. Treatment emphasizes functional rehabilitation—restoring normal movement patterns through exercise and postural retraining. Patients often feel “mostly better” but objective measures may still show restrictions requiring correction.
Month 4-6 (Stabilization Phase): For moderate to severe injuries, this extended phase focuses on long-term stability. Residual ligament laxity may require ongoing support through exercise, ergonomic modifications, or periodic maintenance adjustments. Some patients reach maximum medical improvement (MMI) during this period, though severe cases may require 12-18 months.
Important Variables: Age, pre-existing conditions, injury severity, and treatment compliance all affect timeline. A 25-year-old with no prior injuries may achieve stabilization in 8 weeks. A 55-year-old with pre-existing disc degeneration may require 6 months. Neither scenario represents “normal”—both require individualized care plans.
The single greatest predictor of poor long-term outcome is delayed care. Studies consistently show that patients who begin treatment within 72 hours of injury experience better outcomes than those who delay 2+ weeks, even when injury severity is comparable.
When to Seek Chiropractic Care vs. Other Specialists
Chiropractic care excels for neuro-musculoskeletal injuries, but it is not appropriate for all post-accident conditions. Understanding when to seek specialized care ensures optimal outcomes.

Ideal for Chiropractic Management:
Requires Co-Management or Referral:
Red Flags Requiring Immediate Medical Attention:
The best trauma-focused chiropractors maintain referral networks and recognize the limitations of their scope. Collaborative care—integrating chiropractic, medical, and rehabilitative specialties—produces superior outcomes for complex cases.
Frequently Asked Questions: Chiropractic Care for Auto Injuries
Is chiropractic care safe for patients who have had previous back surgery?
Yes, but with important caveats. Post-surgical patients require modified techniques that avoid the fusion sites or instrumented segments. Many chiropractors are trained in gentle, low-force methods specifically designed for post-operative cases. The key is comprehensive consultation including review of surgical notes and current imaging. In some cases, adjacent segment degeneration (deterioration of vertebrae above or below the fusion) occurs, which chiropractic care can help manage conservatively.
What is the physiological cause of the “popping” sound during an adjustment?
The audible release, called cavitation, occurs when a spinal joint is gapped rapidly, causing dissolved gases (primarily nitrogen) in the synovial fluid to form bubbles—a process called tribonucleation. This is similar to opening a carbonated beverage. The sound itself has no therapeutic value; it’s merely a byproduct of restoring joint motion. Some highly effective adjustment techniques produce no sound at all.
How does non-surgical spinal decompression differ from standard traction?
Traditional traction applies continuous pulling force, which often triggers protective muscle spasm that limits effectiveness. Modern decompression therapy uses computer-controlled intermittent traction with specific angle variations tailored to the patient’s condition. The cycling between decompression and partial relaxation prevents the spasm response while creating negative intradiscal pressure. This negative pressure draws herniated disc material back toward the center and promotes nutrient-rich fluid influx for healing.
Can chiropractic adjustments help with non-musculoskeletal issues like acid reflux or asthma?
This is a controversial area. While the nervous system does influence all body functions, and spinal manipulation can affect autonomic nervous system activity, evidence for treating primary systemic diseases through spinal adjustments alone is limited. Some patients report improvements in digestive or respiratory symptoms during chiropractic care, possibly due to reduced thoracic spine restrictions affecting diaphragm function or vagus nerve signaling. However, these conditions should be co-managed with appropriate medical specialists.
What is the difference in education between a Chiropractor (DC) and a Physical Therapist (DPT)?
Both are doctoral-level professionals with overlapping but distinct scopes. Chiropractors complete 4-5 years of graduate education (typically 4,620 hours) focused heavily on spinal biomechanics, differential diagnosis, and manipulative techniques. They are licensed as portal-of-entry providers who can diagnose and order imaging. Physical therapists complete 3 years of doctorate study (typically 3,000 hours) emphasizing rehabilitation, therapeutic exercise, and mobility restoration across all body systems. PTs typically work from physician referrals, though direct access laws vary by state. Both professions offer valuable but complementary skill sets for trauma rehabilitation.
How many sessions are typically required to stabilize a herniated disc?
This varies dramatically based on herniation size, location, patient age, and compliance with home care recommendations. Minor disc bulges with radicular symptoms may respond within 12-20 sessions over 6-8 weeks. Larger herniations requiring decompression therapy typically need 20-30 sessions over 10-12 weeks. Approximately 70-80% of disc herniation patients achieve significant improvement (50%+ pain reduction) with conservative care, avoiding surgery. The remaining 20-30% may require epidural injections or surgical intervention.
Is the Webster Technique safe during all trimesters of pregnancy?
The Webster Technique is a specific sacral adjustment designed to reduce pelvic misalignment and optimize fetal positioning. It is considered safe throughout pregnancy when performed by a chiropractor with advanced training in prenatal care. However, first-trimester adjustments require special precautions, and any high-risk pregnancy (placenta previa, preeclampsia, etc.) should be co-managed closely with the patient’s obstetrician. Most chiropractors use specialized pregnancy pillows or side-lying positions to avoid prone positioning during later trimesters.
When should I seek care after an accident if I don’t have immediate pain?
Immediately or within 72 hours—even without symptoms. Delayed-onset pain is extremely common due to the body’s initial adrenaline surge and inflammatory cascade timing. Soft tissue injuries often don’t produce significant pain until inflammation peaks at 48-72 hours post-injury. More critically, insurance companies use treatment delays as evidence that injuries are unrelated to the accident or “not medically necessary.” Early documentation establishes causation and begins the clock for statute of limitations purposes.
Does insurance cover chiropractic care after a car accident?
In Colorado, your auto insurance Med-Pay coverage (typically $5,000-$10,000) covers chiropractic care regardless of fault. If Med-Pay is exhausted, health insurance secondary coverage may apply, though many auto injury specialists accept attorney liens rather than billing health insurance to avoid jeopardizing personal injury claims. Always verify your specific policy provisions, as coverage details vary. Most trauma-focused practices offer free insurance verification consultations before starting treatment.
What should I bring to my first appointment after an accident?
Bring: (1) Accident/police report, (2) Insurance information (auto and health), (3) Photos of vehicle damage and visible injuries, (4) List of current symptoms with onset timeline, (5) Any medical records from ER visits or prior care, (6) Attorney contact information if retained, (7) List of current medications, (8) Prior injury history. This documentation allows comprehensive assessment and proper claim coordination from day one.
Final Resources & Next Steps
Understanding your injury is the first step toward comprehensive recovery. The second step is connecting with qualified providers who specialize in the unique challenges of auto injury rehabilitation—from advanced diagnostics to insurance documentation.
Locate an Experienced Provider in Your Area »
Don’t navigate this process alone. Our featured providers offer complimentary consultations to review your case, explain your insurance coverage options, and develop a personalized recovery plan based on your specific injuries.
Find a Featured Provider Who Specializes in Auto Injuries
No upfront costs. No referral required. All providers accept Colorado Med-Pay and Attorney Lien arrangements.