

Car Accident Treatments
Auto Collision Injury Treatment: Medical Standards & Rehabilitation Protocols
Auto collision injury treatment encompasses the specialized medical protocols designed to diagnose and rehabilitate soft tissue damage, ligamentous instability, and neurological trauma resulting from vehicular impacts. Unlike emergency medicine—which prioritizes life-threatening conditions—collision injury care addresses delayed-onset musculoskeletal and neurological symptoms that often emerge 24-72 hours post-impact. These protocols integrate advanced diagnostic imaging, multi-disciplinary therapeutic interventions, and medical-legal documentation standards required for both clinical recovery and insurance claim substantiation.
The complexity of post-collision injuries requires providers trained in biomechanical assessment, AMA impairment rating methodologies, and trauma-informed care delivery. Standard primary care or emergency room evaluations typically lack the diagnostic precision needed to detect ligamentous laxity, early-stage disc herniations, or subtle neurological deficits that characterize whiplash-associated disorders.
Table of Contents[Hide][Show]
Medical-Legal Documentation & Injury Claims+−
- AMA Impairment Rating Standards
- Narrative Reports and Causation Analysis
- The Role of Independent Medical Examinations
- Navigating Auto Insurance & Medical Liens in Colorado
- Personal Injury Protection (PIP) Coverage
- Medical Payment (MedPay) Benefits
- Letters of Protection and Medical Liens
- Colorado Statutes and Claim Timelines
- Frequently Asked Questions: Post-Collision Injury Care
- Clinical Disclaimer
Specialized Treatment Modalities Available in Colorado
Colorado Car Accident Chiro offers evidence-based therapeutic interventions specifically designed for post-collision rehabilitation. Each modality addresses distinct injury patterns commonly observed in vehicular trauma cases:

Complete Car Accident Treatment Protocols – Comprehensive initial evaluation and phased care planning

Spinal Decompression Therapy for Disc Injuries – Non-surgical treatment for herniated or bulging discs

Laser Therapy for Soft Tissue Healing – Photobiomodulation to accelerate cellular repair

Percussor Therapy for Deep Tissue Rehabilitation – Mechanized tissue mobilization for chronic tension
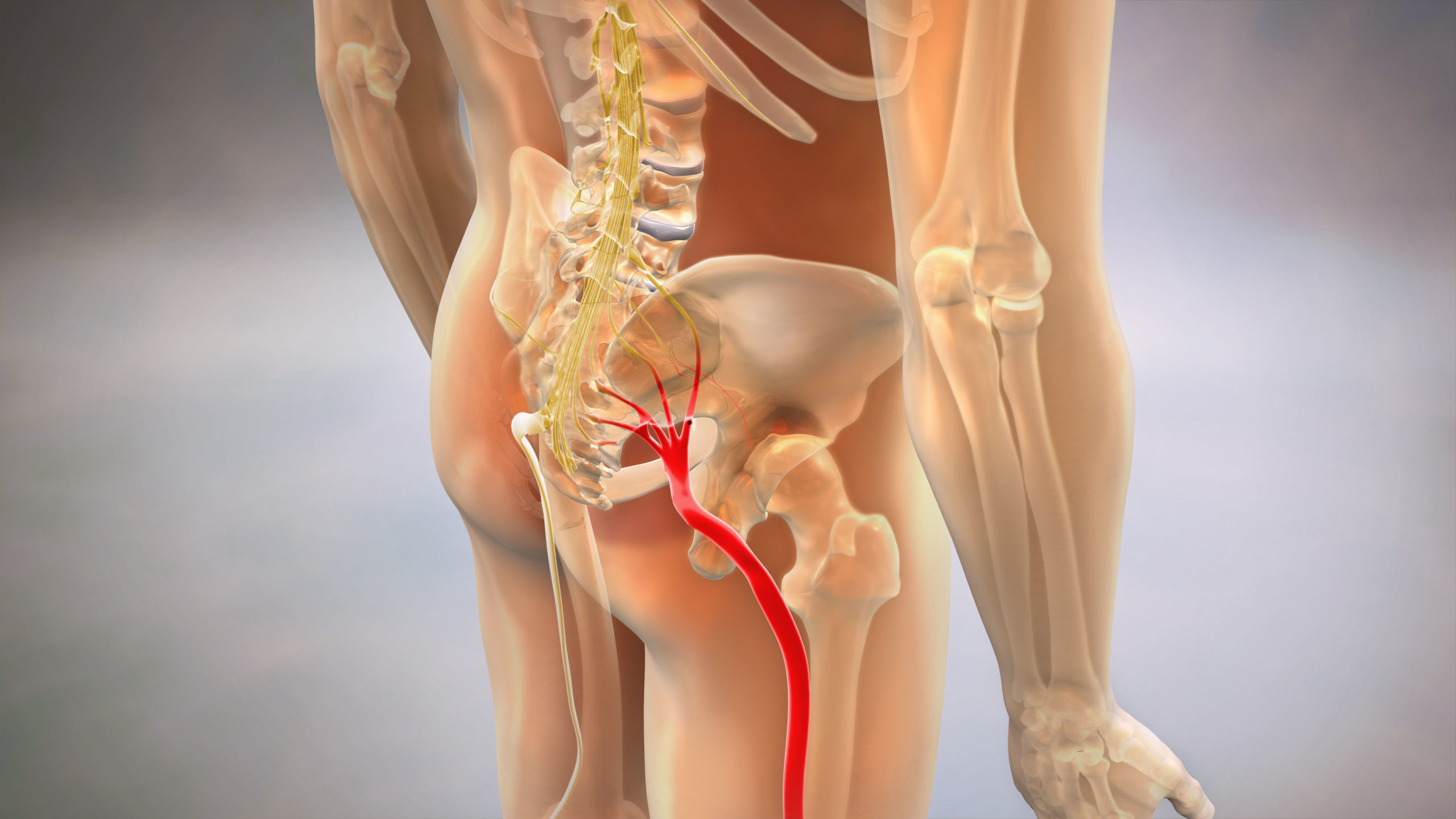
Sciatica Pain Relief After Collision Impact – Targeted protocols for radiating lower extremity symptoms

Chiropractic Adjustments for Spinal Alignment – Biomechanical correction of vertebral subluxations
Auto Collision Injury Specialist Near You
Understanding Post-Collision Injury Mechanisms
Vehicular collisions generate forces that exceed normal physiological tolerances of human tissue. The mechanism of injury differs significantly from other musculoskeletal conditions due to sudden acceleration-deceleration dynamics.
Whiplash Biomechanics
During rear-end collisions, the torso accelerates forward while the head initially remains stationary due to inertia. This creates a hyperextension motion followed by compensatory hyperflexion—often occurring in under 500 milliseconds. The cervical spine experiences force loads that can strain ligaments, facet joint capsules, and intervertebral discs beyond their elastic limit. Research indicates that impacts as low as 5-8 mph can generate sufficient force to cause soft tissue injury, even when vehicle damage appears minimal.
Ligamentous Laxity and Instability
Unlike muscle strains that typically heal within 6-8 weeks, ligament damage may result in permanent elongation. Ligaments lack the vascular supply of muscle tissue, making complete healing difficult once the elastic threshold is exceeded. This creates chronic instability in spinal segments, leading to abnormal motion patterns detectable through specialized imaging such as Digital Motion X-Ray (DMX). Static X-rays and standard MRIs frequently fail to capture this functional instability.
Neurological Involvement
The brainstem and upper cervical nerve roots are particularly vulnerable during whiplash events. Disruption of cervical proprioceptors can cause dizziness, balance disturbances, and visual tracking difficulties—symptoms often misattributed to psychological stress rather than recognized as neuro-vestibular dysfunction. Additionally, direct compression or inflammatory irritation of nerve roots may produce radiating pain, paresthesias, or motor weakness in the upper extremities.
The Phased Treatment Timeline
Evidence-based collision injury care follows a structured progression based on tissue healing phases and functional restoration milestones.
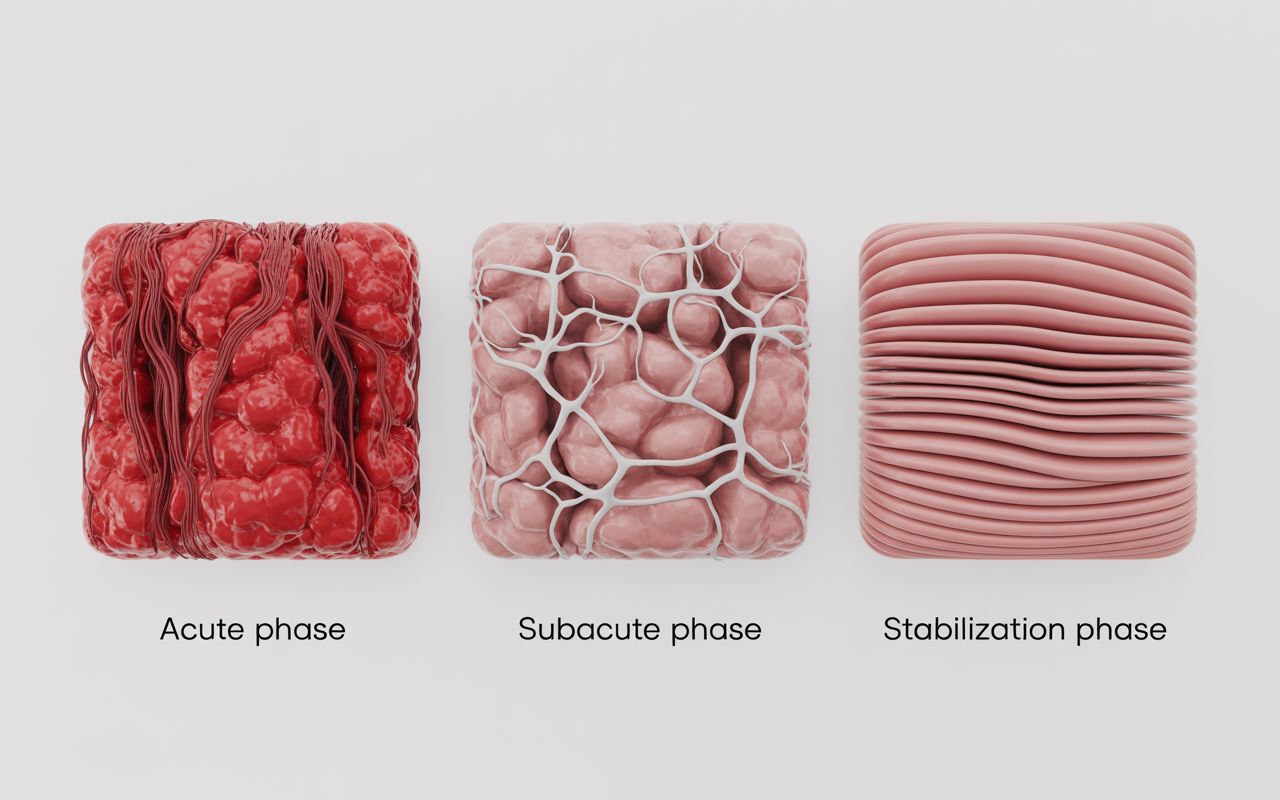
Acute Phase (0-14 Days Post-Impact)
Initial care priorities include inflammation management, pain modulation, and prevention of chronic pain patterns. Treatment during this window typically involves gentle mobilization, cryotherapy, and neuromuscular re-education. Aggressive manipulation is contraindicated during the acute inflammatory phase. Diagnostic imaging is performed to rule out fractures, dislocations, or other contraindications to manual therapy.
Early intervention during this phase significantly reduces the likelihood of chronic pain development. Delayed treatment beyond 14 days correlates with increased risk of long-term disability according to research published in the Journal of Orthopaedic & Sports Physical Therapy.
Subacute Phase (2-12 Weeks)
As acute inflammation subsides, treatment shifts toward restoring range of motion, rebuilding muscular endurance, and correcting compensatory movement patterns. This phase integrates active rehabilitation exercises, manual therapy, and modalities such as laser therapy or spinal decompression. Progressive loading principles guide the return to normal activities.
Patients often experience fluctuating symptoms during this phase as scar tissue remodels and neurological pathways recalibrate. Consistent therapeutic intervention prevents the formation of adhesions and maintains optimal tissue extensibility.
Chronic Management (Beyond 12 Weeks)
For cases involving permanent impairment or residual symptoms, ongoing maintenance care may be necessary. This includes periodic adjustments, home exercise programs, and ergonomic modifications. Medical-legal documentation during this phase establishes maximum medical improvement (MMI) and quantifies permanent functional deficits using AMA impairment rating guidelines.
Advanced Diagnostic Technologies in Trauma Care
Accurate diagnosis of collision-related injuries requires imaging modalities that exceed the capabilities of standard emergency room protocols.
Digital Motion X-Ray (DMX)
DMX technology captures real-time fluoroscopic images as the patient moves through active ranges of motion. This functional imaging reveals abnormal spinal mechanics, ligamentous instability, and segmental hypermobility that remain invisible on static X-rays. The technology is particularly valuable for documenting whiplash-associated disorders in medical-legal contexts.
Traditional static imaging captures only a single moment in time. DMX provides objective evidence of dynamic dysfunction, making it the gold standard for detecting ligament damage in personal injury cases. Providers certified in DMX interpretation can identify instability patterns that correlate with patient symptom reports and functional limitations.
MRI vs. X-Ray in Soft Tissue Assessment
Magnetic Resonance Imaging excels at visualizing disc herniations, spinal cord compression, and muscle edema. However, MRI requires the patient to remain motionless in a supine position—a posture that may not replicate the mechanical stresses that produce symptoms during daily activities. X-ray imaging, while limited in soft tissue visualization, provides superior detail of bony alignment and arthrokinematics.
Comprehensive diagnostic protocols often utilize both modalities. MRI identifies structural pathology, while motion studies reveal functional impairment. This combination provides the clinical and legal documentation necessary for complex injury claims.
Neurological and Vestibular Testing
Post-concussion symptoms and vestibular dysfunction require specialized assessment beyond standard neurological exams. Balance testing, oculomotor screening, and cognitive assessments identify deficits that emergency departments rarely evaluate. These subtle impairments significantly impact quality of life but often go unrecognized without targeted evaluation.
Multi-Disciplinary Treatment Modalities
Effective collision injury rehabilitation requires integration of multiple therapeutic approaches, each addressing specific aspects of tissue healing and functional restoration.
Chiropractic Spinal Manipulation
Manual adjustments restore proper segmental motion to vertebrae restricted by joint dysfunction or muscle guarding. High-velocity, low-amplitude thrusts create cavitation within joint spaces, reducing pain through mechanoreceptor stimulation and improving proprioceptive input. Manipulation is contraindicated in cases of acute fracture, spinal cord compression, or severe osteoporosis.
Physical Rehabilitation and Therapeutic Exercise
Progressive resistance training rebuilds muscular strength depleted during the acute injury phase. Neuromuscular re-education exercises retrain movement patterns disrupted by pain avoidance behaviors. Functional capacity evaluations measure objective improvement and identify remaining deficits. This component is essential for patients returning to physically demanding occupations.
Soft Tissue Therapies
Myofascial release, instrument-assisted soft tissue mobilization, and percussor therapy address adhesions, trigger points, and chronic tension patterns. These techniques improve tissue extensibility and reduce pain referral patterns. When combined with other modalities, soft tissue work accelerates recovery and prevents compensatory injuries.
Laser Therapy and Regenerative Modalities
Class IV laser therapy delivers photonic energy to damaged tissues, stimulating cellular metabolism and accelerating healing. Research demonstrates efficacy in reducing inflammation, improving microcirculation, and modulating pain signaling. Non-invasive and well-tolerated, laser therapy complements manual therapies without adverse effects.
Spinal Decompression
Mechanical decompression applies controlled axial distraction to the spine, creating negative pressure within intervertebral discs. This promotes the retraction of herniated disc material and increases nutrient diffusion into avascular disc tissue. Decompression protocols are indicated for radiculopathy, disc bulges, and chronic discogenic pain unresponsive to conservative care.
Medical-Legal Documentation & Injury Claims

Proper clinical documentation serves dual purposes: guiding treatment decisions and substantiating insurance claims. Inadequate documentation is the leading cause of claim denials in auto injury cases.
AMA Impairment Rating Standards
The AMA Guides to the Evaluation of Permanent Impairment provide standardized methodology for quantifying functional deficits. These ratings directly influence settlement values and disability determinations. Providers trained in AMA guidelines ensure that clinical findings translate accurately into legal contexts.
Impairment ratings consider range of motion loss, neurological deficits, and structural pathology. Objective measurements and validated testing protocols are essential. Subjective pain reports alone are insufficient for impairment rating purposes.
Narrative Reports and Causation Analysis
Detailed narrative reports establish the causal relationship between the collision event and the diagnosed injuries. These documents explain the biomechanical plausibility of injuries relative to the forces involved, address gaps in treatment timelines, and provide prognosis statements. Insurance adjusters and attorneys rely on these reports when evaluating claims.
Effective narrative reports synthesize diagnostic findings, clinical examination data, and treatment response. They address defense arguments such as pre-existing conditions or delayed treatment by providing clinical reasoning grounded in peer-reviewed literature.
The Role of Independent Medical Examinations
Insurance companies often request Independent Medical Examinations (IMEs) to challenge treating provider opinions. Understanding IME tactics and maintaining meticulous documentation protects patients from unfair claim denials. Treating providers should anticipate IME scrutiny and document accordingly from the initial evaluation forward.
Navigating Auto Insurance & Medical Liens in Colorado
Colorado’s insurance laws create specific opportunities and obligations for collision injury patients.
Personal Injury Protection (PIP) Coverage
Colorado requires minimum PIP coverage, which pays for medical expenses regardless of fault. PIP typically covers initial treatment costs up to policy limits. Understanding PIP benefits prevents patients from incurring unnecessary out-of-pocket expenses while claims are processed. Providers experienced with PIP billing streamline this process.
Medical Payment (MedPay) Benefits
MedPay functions similarly to PIP but may offer higher coverage limits depending on the policy. Unlike health insurance, MedPay applies specifically to auto accident injuries without deductibles or copays in most cases. Patients should verify MedPay availability before utilizing health insurance, which may trigger subrogation claims.
Letters of Protection and Medical Liens
When insurance benefits are exhausted or disputed, Letters of Protection allow treatment to continue while the claim is resolved. The provider agrees to defer payment until settlement, assuming the financial risk. This ensures that patients receive necessary care regardless of immediate ability to pay.
Medical lien arrangements require clear documentation of treatment necessity and costs incurred. Providers working on liens must maintain transparent communication with patients and their legal representatives regarding outstanding balances and settlement expectations.
Colorado Statutes and Claim Timelines
Colorado law imposes a three-year statute of limitations for personal injury claims arising from auto collisions. However, insurance companies may impose shorter deadlines for reporting injuries and submitting treatment claims. Prompt medical evaluation and consistent treatment create stronger documentation trails and prevent administrative denials.
When to Seek Specialized Care vs. General Practice

Not all collision injuries require specialized trauma care. However, specific symptoms and circumstances indicate the need for providers with advanced training in post-collision injury management.
Red Flag Symptoms Requiring Immediate Evaluation
Severe headaches, loss of consciousness, altered mental status, or progressive neurological symptoms require emergency evaluation to rule out traumatic brain injury or spinal cord compromise. Numbness, weakness, or bowel/bladder dysfunction indicate potential nerve root or spinal cord involvement requiring urgent imaging.
The ER Gap: What Emergency Departments Miss
Emergency medicine appropriately focuses on life-threatening conditions. Soft tissue injuries, ligamentous instability, and mild traumatic brain injuries often receive minimal evaluation beyond basic X-rays. Patients are commonly discharged with pain medication and instructions to follow up “if symptoms worsen”—creating a dangerous gap in care.
Studies show that delayed treatment correlates with worse long-term outcomes. Seeking specialized evaluation within 72 hours of collision, even when the ER provides clearance, ensures that subtle injuries receive appropriate attention before chronic patterns develop.
Provider Vetting: Credentials That Matter
Effective collision injury care requires specific training beyond general chiropractic or physical therapy licensure. Key credentials include DMX certification, AMA impairment rating training, and experience with medical-legal documentation. Providers affiliated with trauma networks or holding advanced whiplash certifications demonstrate commitment to evidence-based, specialized care.
Patients should inquire about a provider’s experience with auto injury cases specifically, not just general musculoskeletal care. The clinical approach to collision injuries differs substantially from sports injuries or chronic degenerative conditions.
Frequently Asked Questions: Post-Collision Injury Care
How long should I wait to seek treatment after a car accident?
Ideally, specialized evaluation should occur within 72 hours of the collision, even if emergency room assessment found no fractures or immediate injuries. The inflammatory process following soft tissue trauma creates a progressive symptom pattern that may not manifest fully during the first 24 hours. Early intervention during the acute phase significantly improves long-term outcomes and creates proper documentation for insurance claims.
Waiting beyond two weeks to initiate treatment may complicate insurance claims, as adjusters often question the causal relationship between the collision and delayed-reported injuries.
What are the latent symptoms of whiplash I should watch for?
Common delayed-onset symptoms include neck stiffness that worsens over 48-72 hours, headaches originating from the base of the skull, dizziness or balance disturbances, difficulty concentrating or memory problems, radiating pain into the shoulders or arms, and visual disturbances. These symptoms reflect the progression of tissue inflammation and neurological irritation that develops as the body’s initial stress response subsides.
Any symptom that emerges or worsens within two weeks of collision should be evaluated by a provider experienced in trauma care, as these may indicate injuries requiring specific therapeutic intervention.
Does car insurance cover chiropractic care and physical therapy?
In Colorado, Personal Injury Protection (PIP) and Medical Payment (MedPay) coverage typically includes chiropractic and physical therapy services for collision-related injuries. These benefits apply regardless of fault and do not require deductibles in most policies. Coverage limits vary by policy, but initial treatment is generally covered without out-of-pocket expense to the patient.
At-fault party liability claims may also cover medically necessary treatment. Providers experienced with auto injury billing handle these insurance processes directly, minimizing administrative burden on patients.
What is the difference between a medical lien and paying out of pocket?
A medical lien is a legal agreement allowing treatment to proceed when insurance benefits are exhausted or disputed, with payment deferred until case settlement. The patient receives necessary care immediately without upfront payment. The provider accepts payment risk in exchange for treating the injury appropriately. This prevents gaps in treatment that could harm both recovery and claim value.
Paying out of pocket requires immediate payment at the time of service. While this eliminates lien arrangements, most collision injury patients lack the resources to fund comprehensive care without insurance or lien arrangements, particularly when injuries require months of treatment.
How do doctors objectively prove soft tissue injuries for settlements?
Objective documentation includes functional imaging such as Digital Motion X-Ray showing abnormal spinal mechanics, range of motion measurements demonstrating loss compared to normative data, muscle testing revealing strength deficits, and AMA impairment ratings quantifying permanent functional loss. Comprehensive examination findings, treatment records showing consistent care, and causation narrative reports linking injuries to the collision mechanism all contribute to substantiating soft tissue injury claims.
Subjective pain reports alone rarely suffice for insurance claim acceptance. Providers trained in medical-legal documentation understand which examination findings and diagnostic tests carry weight in claim evaluations.
Can I receive treatment if I do not have health insurance?
Yes. Auto collision injuries are typically covered by auto insurance, not health insurance. PIP and MedPay benefits apply regardless of whether you carry health insurance. When these benefits are exhausted and the at-fault party’s insurance is disputed, Letter of Protection arrangements allow treatment to continue with payment deferred until claim resolution.
Providers specializing in auto injury care routinely work with uninsured patients through these mechanisms. Health insurance status should not delay seeking necessary treatment following a collision.
What therapies are best for post-accident headaches and dizziness?
Post-collision headaches often originate from cervical spine dysfunction, muscle tension, or mild traumatic brain injury. Treatment typically includes cervical adjustments to restore proper neck mechanics, soft tissue therapy targeting suboccipital muscles, vestibular rehabilitation for balance disturbances, and laser therapy to reduce inflammation in affected tissues.
Dizziness specifically may require neuro-vestibular assessment to identify inner ear involvement or proprioceptive deficits. Persistent headaches or dizziness beyond two weeks warrant comprehensive neurological evaluation to rule out concussion or other intracranial injuries. These symptoms should never be dismissed as “normal” recovery discomfort.
Clinical Disclaimer
The information provided on this page is for educational purposes and does not constitute medical advice, diagnosis, or treatment recommendations. Individual collision injuries vary significantly based on impact dynamics, pre-existing conditions, and patient-specific factors. Proper evaluation by a licensed healthcare provider is necessary to determine appropriate treatment protocols. No content on this page guarantees specific recovery outcomes or settlement values. Colorado Car Accident Chiro maintains medical and legal compliance with all applicable Colorado statutes and healthcare regulations.