

Chiropractic Adjustments
Chiropractic Adjustments: A Comprehensive Guide to Spinal Manipulation Therapy
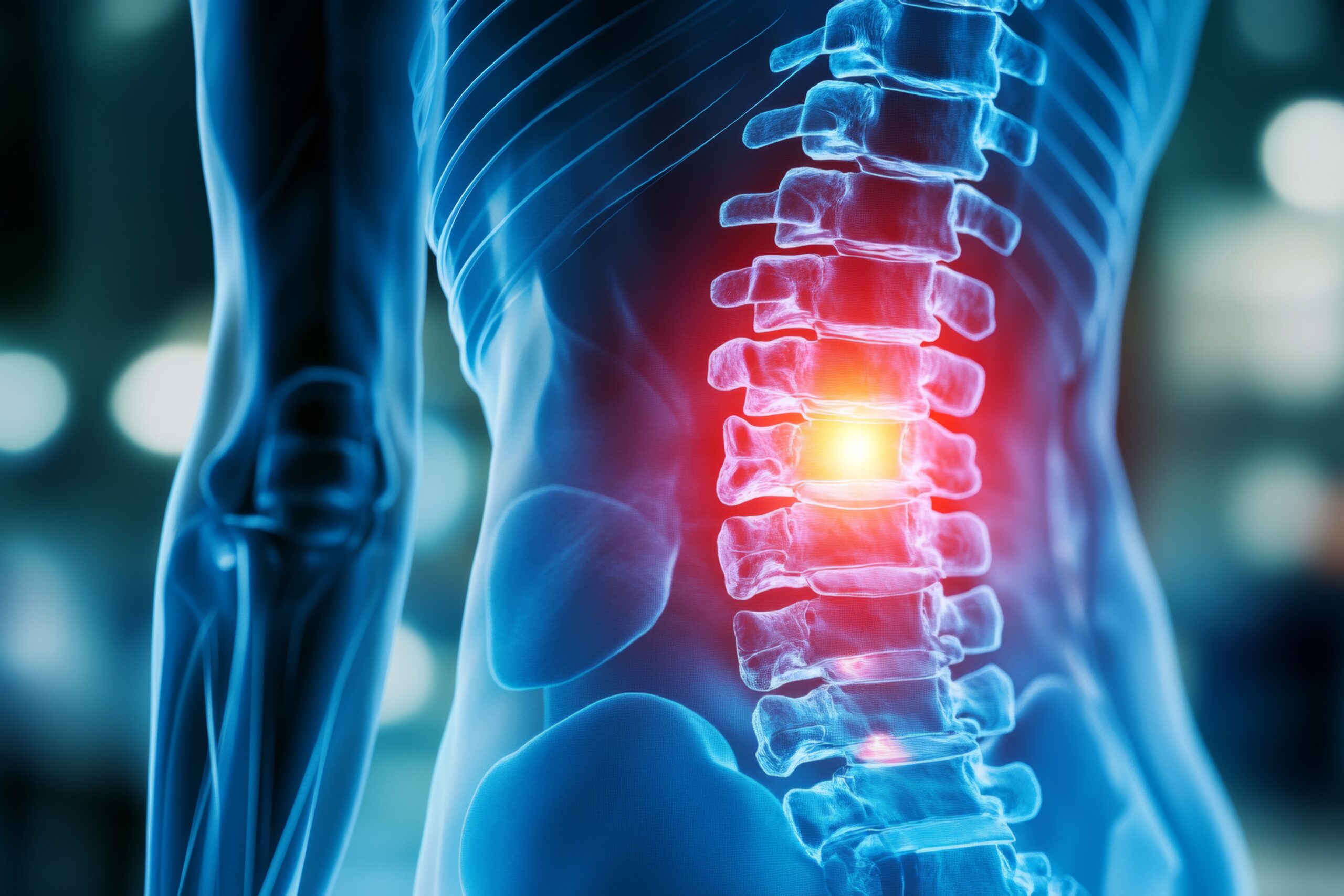
A chiropractic adjustment, also known as spinal manipulation, is a controlled therapeutic force applied to a spinal joint to restore proper biomechanical function and neurological communication. The characteristic “popping” sound—called tribonucleation—occurs when nitrogen gas bubbles are released from the synovial fluid within the joint capsule. This audible release is not bone cracking, but rather a pressure change within the joint space that accompanies the restoration of normal range of motion.
Chiropractic adjustments are distinguished from other manual therapies by their high-velocity, low-amplitude (HVLA) thrust technique, which targets specific spinal segments to address joint dysfunction, reduce pain, and improve proprioceptive signaling between the nervous system and musculoskeletal structures.
Table of Contents[Hide][Show]
Specialized Chiropractic Treatment Pathways in Colorado
Depending on your injury mechanism and symptom presentation, different therapeutic modalities may complement your adjustment protocol. Our clinic specializes in post-trauma rehabilitation and evidence-based spinal care:


Comprehensive Car Accident Chiropractic Treatment – For multi-system trauma recovery and insurance documentation
Spinal Decompression Therapy – For disc herniation and nerve root compression with DMX-guided protocols

Laser Therapy for Soft Tissue Injuries – For inflammation reduction and accelerated cellular repair

Percussor Therapy for Muscle Tension -For deep trigger point release and fascial restrictions
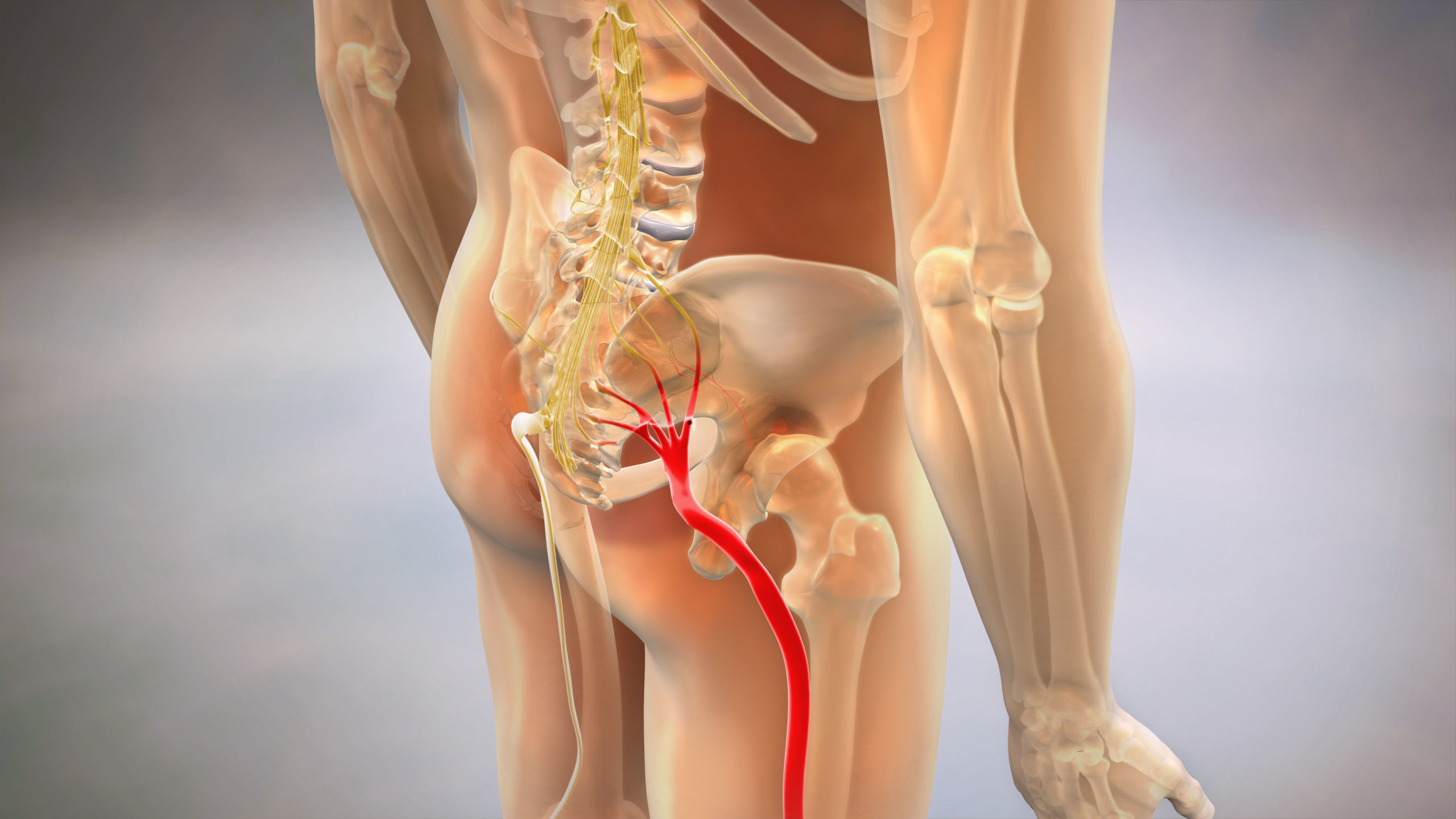
Sciatica Pain Relief Programs – For radiculopathy and nerve compression syndromes
Each treatment pathway is customized based on diagnostic imaging findings and functional capacity evaluations to ensure both symptomatic relief and objective documentation of recovery.
Find a Chiropractic Treatment Specialist Near You
The Science Behind Spinal Manipulation
The therapeutic effect of chiropractic adjustments operates through multiple physiological pathways. When a spinal joint becomes hypomobile—whether due to trauma, inflammation, or degenerative changes—the surrounding mechanoreceptors fail to transmit accurate proprioceptive information to the central nervous system. This creates a “sensory mismatch” that the brain interprets as pain or dysfunction.
The HVLA thrust temporarily separates the joint surfaces, stimulating Type I and Type II mechanoreceptors while simultaneously inhibiting nociceptive (pain) signals through the Gate Control Theory mechanism. This neurological “reset” restores normal joint motion and reduces muscle guarding patterns that perpetuate dysfunction.
The tribonucleation phenomenon itself is a byproduct of cavitation—when the joint space rapidly expands, dissolved gases in the synovial fluid form bubbles that produce the characteristic audible pop. Research using real-time MRI imaging has confirmed that the sound occurs at the exact moment of joint separation, and that subsequent “popping” cannot occur until gases redissolve into the fluid, typically within 20-30 minutes.
Beyond the mechanical effect, spinal manipulation triggers the release of endogenous opioids and reduces inflammatory cytokine production, providing both immediate and sustained pain relief without pharmaceutical intervention.
Types of Chiropractic Adjustment Techniques
Not all adjustments are performed identically. Chiropractors are trained in multiple techniques, each suited to different injury patterns and patient tolerances:
Diversified Technique is the most commonly used method, involving a high-velocity thrust to specific spinal segments identified through palpation and motion analysis. The provider uses body positioning and precise hand contacts to isolate the dysfunctional joint.
Gonstead Method emphasizes detailed analysis using instrumentation (nervoscope) and full-spine X-rays to identify subluxations. Adjustments are delivered from specific angles using a pelvic bench or cervical chair to maximize segmental specificity.
Activator Method utilizes a spring-loaded instrument that delivers a controlled, low-force impulse to the spine. This technique is often preferred for geriatric patients, acute inflammation cases, or individuals with osteoporosis where manual thrusting may be contraindicated.
Drop-Table Technique (Thompson Technique) uses a specialized table with sections that drop slightly during the thrust. The dropping motion assists the adjustment force while reducing the amount of manual pressure required.
Flexion-Distraction is a gentle, non-thrusting technique primarily used for disc herniations and spinal stenosis. The table mechanically flexes and distracts the spine while the provider applies targeted pressure to the affected segment.
Technique selection is based on diagnostic findings, patient presentation, and contraindications identified during the clinical examination.

Clinical Indications for Chiropractic Care
Chiropractic adjustments are clinically indicated for a range of neuromusculoskeletal conditions, particularly those involving joint dysfunction or soft tissue injury:
Acute Conditions: Cervical acceleration-deceleration (whiplash) injuries, acute low back strain, rib subluxations, thoracic outlet syndrome, and post-traumatic headaches.
Chronic Conditions: Degenerative disc disease, facet joint syndrome, chronic cervicogenic headaches, lumbar instability, and failed back surgery syndrome.
Auto Injury Presentations: Motor vehicle accidents create unique injury patterns characterized by ligamentous laxity, delayed symptom onset, and objective findings that may not appear on static imaging. Digital Motion X-Ray (DMX) is often necessary to visualize ligament instability that would otherwise go undetected.
Contraindications include: Acute fractures, spinal infections (osteomyelitis, discitis), active malignancy involving the spine, severe osteoporosis with compression fracture risk, and vertebrobasilar insufficiency. Relative contraindications require modified techniques or referral to appropriate specialists.
The key clinical distinction is between subluxation complex (reversible joint dysfunction) and structural pathology (herniation, stenosis, fracture). Proper diagnosis through imaging and orthopedic testing determines appropriateness for adjustive care.
Adjustment vs. Mobilization: Understanding the Difference
Patients often confuse chiropractic adjustments with physical therapy mobilization. While both address joint dysfunction, the biomechanical approach differs significantly:
Chiropractic Adjustment (HVLA): A quick, controlled thrust delivered to the end range of motion, resulting in joint cavitation. The speed of the thrust is what allows the joint surfaces to separate beyond their normal physiological barrier without tissue damage.
Physical Therapy Mobilization: Graded oscillatory movements (Maitland Grades I-IV) applied within the joint’s available range. These slower, rhythmic pressures increase mobility through repetition rather than cavitation.
Grade I-II mobilizations are used for pain relief and do not reach the end range of motion. Grade III-IV mobilizations stretch the joint capsule but stop short of the thrust velocity required for cavitation. Grade V mobilization is equivalent to a chiropractic adjustment and requires specialized training.
The choice between adjustment and mobilization depends on tissue tolerance, inflammation levels, and patient preference. Post-traumatic cases with acute ligament injury may require mobilization initially before progressing to adjustive care once stability improves.
Safety, Risks, and Evidence-Based Outcomes
Chiropractic adjustments are considered safe when performed by licensed providers following appropriate diagnostic protocols. Large-scale studies estimate serious adverse events occur in approximately 1 in 2 million cervical adjustments, primarily vertebrobasilar artery dissection in patients with pre-existing vascular abnormalities.
Common Mild Side Effects: Temporary soreness (24-48 hours), muscle fatigue, or localized tenderness at the adjustment site. These effects are comparable to post-exercise soreness and resolve without intervention.
Special Populations:
Pediatric: Adjustments for children use minimal force (often no more pressure than checking a tomato for ripeness). Studies support safety and efficacy for conditions like torticollis and postural dysfunction.
Geriatric: Modified techniques (activator, mobilization) are used for patients with decreased bone density. Pre-adjustment screening for osteoporosis is standard protocol.
Pregnancy: Tables with abdominal cutouts and Webster Technique (for pelvic balance) are safe throughout pregnancy and may reduce labor complications.
Evidence Summary: Systematic reviews consistently show chiropractic care is as effective as or superior to medical management for acute and chronic low back pain, with lower rates of opioid prescribing. For cervical acceleration-deceleration injuries, early chiropractic intervention reduces chronicity and improves long-term functional outcomes.
The Role of Diagnostic Imaging
Appropriate imaging is essential to identify structural pathology and guide treatment planning. However, not all imaging modalities provide the same diagnostic value:
Static X-Ray: Shows bone alignment, disc space height, and degenerative changes but cannot assess ligament integrity or dynamic instability.
Digital Motion X-Ray (DMX): Captures the spine in motion (flexion/extension), revealing excessive segmental motion, ligament laxity, and instability patterns invisible on static films. This is particularly critical in auto injury cases where soft tissue damage exceeds visible structural damage.
MRI: The gold standard for disc herniation, nerve compression, and soft tissue pathology. Required when radicular symptoms or neurological deficits are present.
CT Scan: Superior for fracture detection and bony detail but offers no soft tissue visualization.
Colorado insurance regulations, including Colorado Med-Pay mandates, typically cover medically necessary diagnostic imaging when ordered by a licensed provider for injury documentation and treatment planning.
Chiropractic Adjustments in Colorado Auto Injury Cases
Colorado operates under a modified comparative negligence system, meaning injury documentation is critical for insurance claims. Auto injury victims face unique challenges:
The “Invisible Injury” Problem: Symptoms like dizziness, brain fog, and delayed-onset pain lack objective findings on standard emergency department exams, leading to insurance denial or claim devaluation.
Objective vs. Subjective Findings Comparison:
| Subjective Findings | Objective Findings |
| Patient-reported pain levels | Measurable loss of range of motion (ROM) |
| Descriptions of “stiffness” | Positive orthopedic tests (Spurling’s, SLR) |
| Self-reported disability | DMX documentation of ligament laxity |
| Symptom journals | Muscle atrophy measurements |
| Pain drawings | AMA impairment ratings |
Objective findings carry legal and insurance weight that subjective complaints do not. Proper documentation through functional capacity evaluations, computerized range-of-motion testing, and advanced imaging creates the evidentiary foundation for claim approval.
Colorado Med-Pay Coverage: Colorado law requires minimum $5,000 Med-Pay coverage on all auto policies. This “no-fault” coverage pays for chiropractic treatment regardless of who caused the accident, removing the immediate cost barrier to care.
Frequently Asked Questions About Chiropractic Adjustments
What actually causes the “popping” sound during a chiropractic adjustment?
The sound is tribonucleation—the formation and collapse of gas bubbles (primarily nitrogen) within the synovial fluid when the joint pressure suddenly decreases. It’s the same physics that causes knuckles to crack, and the presence or absence of the sound does not indicate the quality of the adjustment.
Is it safe to perform chiropractic adjustments on children or the elderly?
Yes, when performed by a licensed chiropractor using age-appropriate techniques. Pediatric adjustments use fingertip pressure only, while geriatric patients receive modified techniques (instrument-assisted or mobilization) to accommodate reduced bone density. Contraindication screening is mandatory for all ages.
How does a chiropractic adjustment differ from physical therapy mobilization?
Adjustments use high-velocity, low-amplitude thrusts that cause joint cavitation, while mobilization uses slower, oscillatory movements within the joint’s existing range. Adjustments target neurological reset and immediate range-of-motion gains; mobilization targets gradual capsular stretching.
Can a chiropractic adjustment help with non-back issues like migraines or digestion?
Cervicogenic headaches (originating from neck dysfunction) respond well to upper cervical adjustments. Digestive claims lack robust evidence. Chiropractors should limit treatment to neuromusculoskeletal conditions within their scope of practice.
What are the signs that a chiropractic adjustment has gone wrong?
Immediate red flags include sudden severe headache, vision changes, slurred speech, loss of coordination, or radiating numbness/weakness. These require emergency evaluation. Normal post-adjustment soreness resolves within 48 hours.
How many sessions are typically required to see permanent results?
Acute conditions (recent injury) typically require 8-12 sessions over 4-6 weeks. Chronic conditions or auto injuries with ligament damage may require 12-24 sessions. “Permanent results” depend on whether the underlying pathology is reversible joint dysfunction versus irreversible structural damage.
Is it possible to adjust your own back safely at home?
Self-manipulation (twisting to “crack” your back) can provide temporary relief but lacks the specificity and controlled force of professional adjustment. Habitual self-manipulation may create joint hypermobility and is not recommended as a substitute for clinical care.