

Percussor Therapy
Clinical Percussor Therapy: Understanding Mechanotransduction for Soft Tissue Rehabilitation
Clinical percussor therapy, also known as variable frequency percussion or mechanotransduction-based soft tissue treatment, is a rehabilitative modality that uses controlled mechanical pressure waves to facilitate connective tissue remodeling at the cellular level. Unlike consumer-grade vibration devices, clinical percussors employ the piezoelectric effect—a biological phenomenon where mechanical force is converted into electrical signaling that instructs collagen fibers to realign, myofascial adhesions to break down, and lymphatic stagnation to resolve.
This technology is distinguished by its ability to penetrate deep fascial layers without the pain associated with manual deep tissue work, making it particularly valuable in acute trauma rehabilitation. The therapeutic mechanism operates through frequency-specific waveforms (typically in the Alpha, Theta, and Delta ranges) that target different tissue depths and physiological responses. In the context of post-collision injuries—especially whiplash, cervical strain, and seatbelt contusions—percussor therapy addresses the “guarded” muscle splinting that occurs when tissues are too inflamed or hypersensitive for traditional manual techniques.
The clinical application of percussor therapy is grounded in mechanobiology research demonstrating that cells respond to mechanical stress by initiating repair cascades. This positions the treatment as a medical necessity for structural rehabilitation rather than a wellness luxury, a distinction critical for personal injury documentation and insurance claims processing.
Table of Contents[Hide][Show]
Treatment Protocols and Integration with Other Modalities+−
- Typical Session Structure
- Integration with Chiropractic Adjustments
- Combination with Spinal Decompression Therapy
- Laser Therapy Synergy
- Treatment Frequency for Acute vs. Chronic Conditions
- Research Evidence and Clinical Validation
- Mechanotransduction Studies
- Fascial Research and Thixotropic Properties
- Clinical Outcomes in Trauma Populations
- Differentiation from Unproven Modalities
- Frequently Asked Questions
Need Percussor-Enhanced Treatment for Your Specific Condition?
Clinical percussor therapy serves as a foundational modality integrated across multiple trauma recovery protocols. Depending on your diagnosis and injury timeline, percussor treatment may be combined with condition-specific approaches:

Comprehensive Car Accident Treatment Protocols – Multi-phase rehabilitation for acute collision injuries
Percussor-Assisted Spinal Decompression Therapy – Combining fascial release with targeted disc rehabilitation

Integrated Laser + Percussor Therapy – Dual-modality approach for inflammation and tissue remodeling
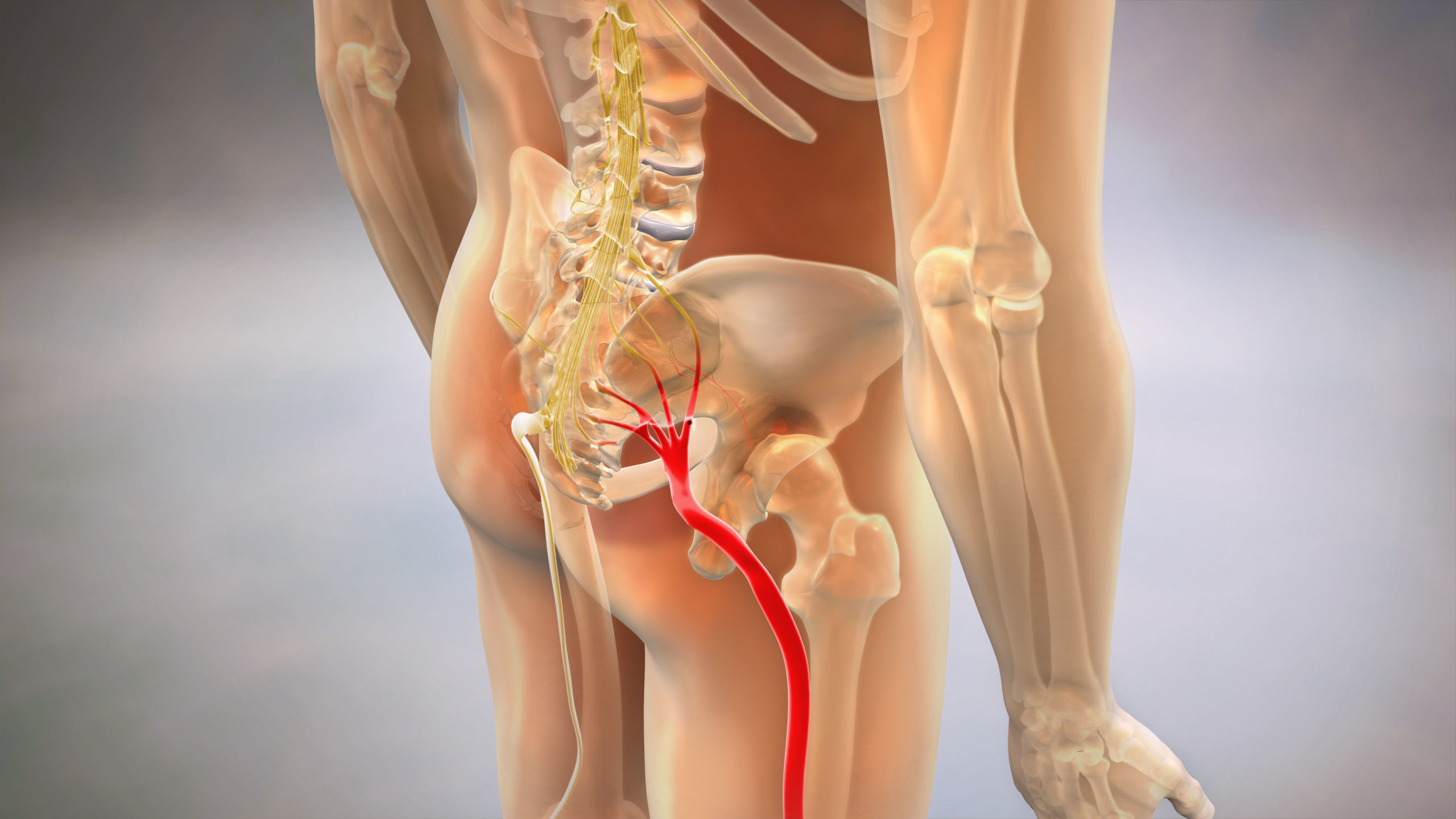
Sciatica Relief Through Fascial Release – Addressing nerve compression via soft tissue intervention

Tissue Preparation for Chiropractic Adjustments – Reducing muscle guarding before joint mobilization
Find a Percussor Therapy Specialist Near You
How Percussor Therapy Works – The Mechanism of Mechanotransduction
The therapeutic foundation of clinical percussion lies in mechanotransduction—the process by which cells convert mechanical stimuli into biochemical signals. When controlled pressure waves from a percussor device contact tissue, they create deformation at the cellular membrane level. This deformation activates mechanoreceptors (specialized proteins embedded in cell walls) that trigger intracellular signaling cascades.
The Piezoelectric Effect in Biological Tissue
Collagen, the primary structural protein in fascia, ligaments, and tendons, exhibits piezoelectric properties. When subjected to mechanical stress, collagen fibers generate small electrical charges. These charges serve as communication signals that instruct fibroblasts (the cells responsible for producing collagen) to begin remodeling damaged or misaligned tissue matrices.
In the context of whiplash or trauma, collagen fibers often become disorganized—laid down in haphazard patterns during the initial inflammatory healing phase. This creates the “stiff” or “locked” sensation patients describe. The frequency-specific mechanical input from a clinical percussor provides the electrical signaling needed to guide fibroblasts in reorganizing these fibers into proper parallel alignment, restoring both strength and flexibility to the tissue.
Differentiation from Massage and Manual Therapy
Traditional massage therapy operates primarily through manual compression and gliding strokes that increase local blood flow and provide temporary muscle relaxation. Manual therapy is surface-oriented and depends on the practitioner’s force application. Clinical percussor therapy, by contrast, delivers non-fatiguing, frequency-controlled mechanical waves that penetrate multiple tissue layers simultaneously.
The key distinction is specificity. A skilled therapist cannot manually replicate the 8-12 Hz Alpha wave frequency required for parasympathetic nervous system activation, nor can they sustain the consistent force needed to reach deep fascial planes in acutely inflamed tissue. The percussor achieves both without causing additional microtrauma or triggering protective muscle guarding—a critical advantage in the first 0-6 months post-injury when tissues are hypersensitive.
The Galvanic Wave Action
Advanced clinical percussors, such as the Erchonia Variable Percussor, utilize a Galvanic wave pattern—a unique waveform that combines percussion with a “carrying” electrical component. This dual-action approach addresses both mechanical adhesions (through direct pressure) and electrochemical stagnation (through charge redistribution in the extracellular matrix). The result is enhanced lymphatic flow, reduced edema, and accelerated breakdown of fibrinous scar tissue that forms at injury sites.
Clinical Percussion vs. Consumer Vibration Devices

The most common barrier to patient acceptance of percussor therapy is the misconception that clinical-grade devices are equivalent to consumer massage guns available at retail stores. While superficially similar in appearance, the technological and therapeutic differences are substantial.
Comparison Table: Clinical Percussor vs. Consumer Massage Guns
| Feature | Clinical Percussor (Erchonia) | Consumer Device (Theragun/Hypervolt) |
| Force Application | Perpendicular percussion (vertical depth) | Oscillating vibration (lateral surface shaking) |
| Frequency Range | Variable: 0.5-12 Hz (Alpha, Theta, Delta) | Fixed: 30-50 Hz (high-frequency vibration only) |
| Tissue Penetration | 3-4 inches (deep fascia, periosteum) | 1-2 inches (superficial muscle layer) |
| Clinical Calibration | Adjustable force and waveform per tissue type | Single-speed or preset levels only |
| Therapeutic Mechanism | Mechanotransduction, piezoelectric signaling | Neuromuscular relaxation via vibration reflex |
| Documentation | Medical-grade tracking for insurance claims | Consumer wellness (not covered by insurance) |
| Primary Use Case | Post-trauma rehabilitation, adhesion breakdown | Post-workout recovery, general muscle soreness |
| Provider Training | Requires certification in frequency protocols | No training required (consumer self-use) |
Why Vibration Alone is Insufficient for Trauma Recovery
High-frequency vibration (30-50 Hz) activates the vibratory inhibition reflex, which temporarily relaxes muscle spindles. This provides short-term relief but does not address the underlying fascial restriction or collagen disorganization. The vibration is also absorbed primarily by the skin and superficial muscle—it lacks the mechanical force needed to deform dense fascial planes or break up fibrinous adhesions.
Clinical percussion, by contrast, uses low-frequency, high-amplitude pressure that bypasses the superficial reflex arc and directly impacts the extracellular matrix. Think of it as the difference between shaking a jar of honey (vibration, which doesn’t change viscosity) versus stirring it with force (percussion, which reduces viscosity through shear stress). The latter is what changes tissue behavior at the structural level.
The Physiology of Fascial Thixotropy – Why Tissue “Unsticks”
One of the most critical concepts in understanding percussor therapy efficacy is thixotropy—the property of certain materials (including fascia) to become less viscous when subjected to stress, then return to a more viscous state at rest.
The Extracellular Matrix as a Gel-Sol System
Fascia is not simply a passive wrapping around muscles; it is a dynamic, hydrated network of collagen fibers, elastin, and ground substance (a gel-like material composed of water, proteins, and polysaccharides). In a healthy state, this ground substance maintains optimal viscosity, allowing muscle fibers to glide smoothly against one another.
After trauma—whether acute impact or chronic repetitive strain—the ground substance becomes more viscous (gel-like), and collagen fibers begin to cross-link inappropriately. This is the biological basis of “adhesions” or “trigger points.” The tissue literally becomes stuck to itself.
How Percussion Induces Thixotropic Shift
When a clinical percussor applies rhythmic pressure to thickened fascia, it introduces shear stress into the ground substance. This mechanical agitation temporarily reduces viscosity, transitioning the tissue from a gel state to a more liquid (sol) state. During this window, fibroblasts can reposition, adhesions can separate, and interstitial fluid can flow more freely.
The frequency of percussion matters here. Research in mechanobiology suggests that 4-8 Hz (Theta wave range) is optimal for inducing thixotropic changes in deep fascia, while higher frequencies (above 12 Hz) primarily affect neuromuscular reflexes without significant structural impact.
Breaking Down Myofascial Adhesions
Adhesions form when fibrinogen (a clotting protein) is deposited at injury sites and subsequently polymerizes into fibrin strands. These strands create cross-links between tissue layers that should normally slide independently. Manual therapy can sometimes stretch these adhesions, but stretching alone does not break the fibrin bonds.
The Galvanic wave action of clinical percussors introduces a dual mechanical and electrical disruption to these bonds. The percussion provides physical shear force, while the electrical component alters the charge distribution that helps stabilize fibrin polymers. This combination accelerates adhesion breakdown more effectively than mechanical force alone, particularly in the cervical spine where manual pressure is often too painful to tolerate in acute phases.
The Three Primary Clinical Applications
While percussor therapy has broad applicability across musculoskeletal conditions, three specific clinical scenarios demonstrate the most significant therapeutic value.
1. Whiplash and Cervical Acceleration-Deceleration Injuries
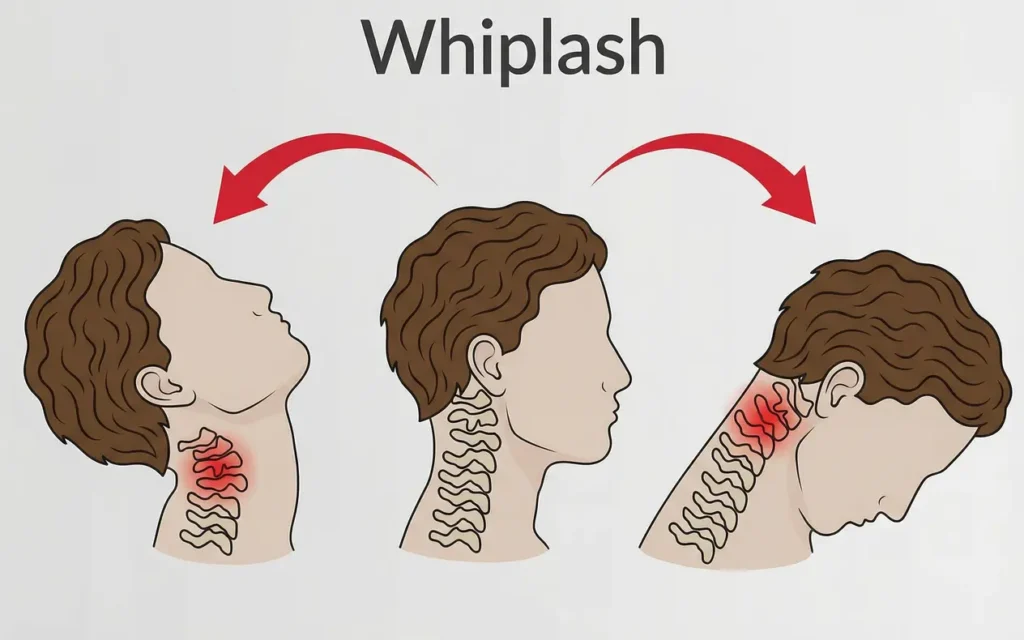
Whiplash creates a unique injury pattern: rapid hyperflexion-hyperextension that tears microscopic fibers in the cervical paraspinal muscles, ligaments, and facet joint capsules. Within 24-48 hours, these tissues respond with protective muscle splinting—an involuntary contraction that limits motion to prevent further damage.
The problem is that this guarding becomes chronic. Even after the initial tear has healed, the muscles remain contracted due to altered proprioceptive signaling and myofascial adhesions. Manual therapy is often intolerable because the tissues are hypersensitive, and aggressive manipulation risks re-injury.
Percussor therapy addresses this by providing non-invasive mechanical input that releases the splinting without triggering pain receptors. The Alpha wave frequency (8-12 Hz) specifically targets the autonomic nervous system, downregulating the sympathetic “threat” response that maintains chronic muscle guarding. Patients often describe the sensation as “soothing” despite the deep tissue penetration—a reflection of parasympathetic activation.
2. Seatbelt Contusions and Lymphatic Stagnation

In moderate to severe collisions, the seatbelt creates a diagonal pressure band across the chest and pelvis. This can cause subcutaneous bruising, fascial shearing, and damage to superficial lymphatic vessels. The result is localized swelling (edema) that persists for weeks or months, creating the “puffy” appearance often visible along the clavicle or anterior shoulder.
Traditional ice and compression provide limited relief because the underlying lymphatic damage impairs fluid drainage. Percussor therapy, particularly when applied with Delta wave frequencies (0.5-4 Hz), stimulates lymphatic vessel contraction—the pumping mechanism that moves interstitial fluid back into circulation.
This application is combined with directional stroking (toward lymph nodes) to guide fluid movement. The treatment is gentle but mechanically precise, addressing the root cause of edema rather than just managing symptoms.
3. Post-Surgical Scar Tissue and Adhesion Management
Patients who have undergone spinal surgery, rotator cuff repair, or abdominal procedures often develop dense scar tissue that limits mobility and causes chronic discomfort. Surgical incisions disrupt fascial planes, and the body’s repair process lays down collagen in a dense, disorganized manner.
Percussor therapy can be introduced 8-12 weeks post-surgery (once primary wound healing is complete) to remodel the scar matrix. The mechanical input encourages fibroblasts to reorganize collagen into more functional patterns, and the piezoelectric signaling supports neovascularization (new blood vessel formation), which improves tissue quality.
This application requires careful frequency selection—typically starting with gentle Theta waves (4-8 Hz) and gradually progressing to more aggressive protocols as tissue tolerance improves. The goal is not to eliminate the scar, but to make it more pliable and less adherent to underlying structures.
Understanding Frequency Modulation – Alpha, Theta, and Delta Waves
Not all percussion is equal. The therapeutic outcome of percussor therapy depends on matching the correct frequency range to the tissue depth, injury phase, and desired physiological response.
Alpha Waves (8-12 Hz) – Autonomic Nervous System Modulation
Alpha frequencies resonate with the brain’s relaxed-but-alert state. When applied to soft tissue, these frequencies stimulate the vagus nerve—the primary conduit of the parasympathetic nervous system. This is particularly valuable in trauma patients who present with chronic hypervigilance, sleep disruption, or anxiety-related muscle tension.
In practical terms, Alpha wave percussion is used on the suboccipital region (base of the skull), upper trapezius, and along the cervical spine to downregulate the stress response. Patients often report feeling “calm” or “grounded” after treatment—a reflection of shifted autonomic tone.
Theta Waves (4-8 Hz) – Deep Fascial Penetration
Theta is the workhorse frequency for structural tissue remodeling. This range penetrates 3-4 inches into tissue, reaching the deep fascial planes, periosteum (bone lining), and ligamentous structures. It is the primary frequency used for breaking up adhesions, improving joint mobility, and addressing chronic stiffness.
Theta waves induce the thixotropic changes discussed earlier, temporarily reducing fascial viscosity to allow remodeling. This frequency is typically applied over the thoracolumbar fascia, iliotibial band, and plantar fascia—areas prone to dense adhesion formation.
Delta Waves (0.5-4 Hz) – Lymphatic Drainage and Edema Resolution
Delta frequencies are the slowest and gentlest. They mimic the natural contraction rate of lymphatic vessels, making them ideal for stimulating fluid movement in edematous tissue. This frequency is used along lymphatic pathways (neck, axilla, groin) and over areas of visible swelling.
Delta wave application is often combined with light manual compression and positional drainage to maximize lymphatic return. The treatment is subtle but highly effective for resolving chronic swelling that resists conventional methods.
Clinical Protocol: Frequency Layering
In practice, a single treatment session often employs multiple frequencies in sequence. A typical protocol for acute whiplash might begin with Delta waves to reduce cervical edema, transition to Theta waves to release paraspinal adhesions, and conclude with Alpha waves to calm the nervous system. This layered approach addresses multiple injury mechanisms simultaneously, accelerating overall recovery.
Treatment Protocols and Integration with Other Modalities
Percussor therapy is rarely used in isolation. Its greatest value emerges when integrated strategically with other rehabilitative interventions.
Typical Session Structure
A standard clinical percussor session lasts 15-20 minutes and follows this general sequence:
- Assessment (2-3 minutes): Identify areas of restriction, guarding, or lymphatic congestion through palpation and range-of-motion testing.
- Frequency Selection (1 minute): Choose the appropriate waveform based on tissue depth, injury phase, and treatment goals.
- Application (10-15 minutes): Systematically treat identified regions using directional strokes, circular patterns, or stationary compression depending on the target tissue.
- Reassessment (2-3 minutes): Re-evaluate range of motion and pain levels to document objective improvement.
Integration with Chiropractic Adjustments
One of the most effective combinations is percussor therapy immediately preceding spinal adjustments. The mechanical release of paraspinal muscle guarding allows for more precise joint mobilization with less force. This reduces patient apprehension, improves cavitation quality (the “pop” associated with joint release), and decreases post-adjustment soreness.
This sequencing is particularly valuable in acute injury cases where traditional “diversified” technique adjustments might be too aggressive. The percussor essentially “prepares” the tissue, allowing the adjustment to target the joint restriction rather than fighting through muscle tension.
Combination with Spinal Decompression Therapy
For patients with disc herniation or radiculopathy (nerve pain), percussor therapy can be applied to the lumbar or cervical paraspinals before or after decompression sessions. The fascial release reduces compressive load on the spine, potentially improving the decompression response.
Additionally, percussor treatment of the psoas muscle (hip flexor) often helps patients tolerate lumbar decompression positioning more comfortably, as psoas tightness is a common compensatory pattern in disc injury cases.
Laser Therapy Synergy
Class IV laser therapy reduces inflammation and stimulates cellular ATP production. When combined with percussor-induced fascial release, the laser’s photonic energy can penetrate more effectively to deeper structures. This dual approach is particularly effective for chronic tendinopathies (Achilles, patellar, rotator cuff) where both adhesions and inflammation contribute to dysfunction.
Treatment Frequency for Acute vs. Chronic Conditions
- Acute Trauma (0-6 weeks post-injury): 3x per week initially, tapering to 2x per week as inflammation resolves. Focus on gentle Delta and Alpha frequencies to manage pain and edema without aggravating tissues.
- Subacute Phase (6 weeks – 3 months): 2x per week with progressive use of Theta frequencies to address developing adhesions and restore functional movement patterns.
- Chronic Conditions (3+ months): 1-2x per week with emphasis on Theta wave remodeling and integration with active rehabilitation exercises to prevent re-adhesion.
Research Evidence and Clinical Validation
While percussor therapy has been utilized in clinical practice for decades, the scientific validation of its mechanisms has accelerated with advances in mechanobiology research.
Mechanotransduction Studies
Peer-reviewed research published in journals such as Nature Reviews Molecular Cell Biology and Journal of Biomechanics has established that mechanical force directly influences cellular behavior. Studies demonstrate that controlled mechanical stress activates integrin receptors (cell surface proteins), which in turn trigger intracellular signaling pathways involving focal adhesion kinase (FAK) and mitogen-activated protein kinase (MAPK).
These pathways regulate collagen synthesis, matrix metalloproteinase production (enzymes that break down adhesions), and inflammatory cytokine expression. In practical terms, this means that mechanical therapy is not merely “breaking up” tissue—it is instructing cells to actively remodel their environment.
Fascial Research and Thixotropic Properties
The Fascia Research Congress, an international collaboration of researchers studying connective tissue, has published findings on the thixotropic behavior of human fascia. Studies using ultrasound elastography (a technique that measures tissue stiffness) show that rhythmic mechanical loading reduces fascial stiffness by 30-40% immediately post-treatment, with sustained improvements when treatment is repeated over multiple sessions.
This research validates clinical observations that percussor therapy produces objective, measurable changes in tissue mechanics—not just subjective pain relief.
Clinical Outcomes in Trauma Populations
While large-scale randomized controlled trials specific to percussor therapy are limited, systematic reviews of “mechanical soft tissue mobilization” (an umbrella term that includes percussion, instrument-assisted techniques, and manual therapy) show consistent benefits for range of motion improvement and pain reduction in musculoskeletal injury populations.
The AMA Guides to the Evaluation of Permanent Impairment recognizes soft tissue mobilization as a medically appropriate intervention for treating myofascial restrictions, providing a legal basis for including percussor therapy in personal injury treatment plans.
Differentiation from Unproven Modalities
It is worth noting that percussor therapy is distinct from modalities with weaker evidence bases, such as static cupping or uncontrolled vibration platforms. The key difference is dose control and physiological specificity. Clinical percussors deliver measurable force at validated frequencies targeting known mechanoreceptor pathways—this positions the treatment within evidence-informed practice rather than speculative wellness trends.
Insurance Coverage and Medical Necessity in Colorado
For patients recovering from auto accidents in Colorado, understanding insurance coverage for percussor therapy is essential for accessing care without financial barriers.
Colorado Med-Pay and PIP Coverage
Colorado law requires auto insurance policies to include Medical Payments Coverage (Med-Pay), which typically provides $5,000-$100,000 in benefits for injury-related medical expenses, regardless of fault. Percussor therapy qualifies as a covered treatment under Med-Pay when it is:
- Prescribed by a licensed provider (DC, MD, DO, PT)
- Medically necessary for treating a documented injury
- Part of a comprehensive treatment plan with objective goals
Unlike wellness massage or maintenance chiropractic care (which are often excluded), percussor therapy is billed as rehabilitative soft tissue mobilization—a recognized medical procedure with CPT codes for insurance documentation.
Documentation Requirements for Personal Injury Claims
Personal injury attorneys representing collision victims prioritize providers who maintain thorough clinical records. For percussor therapy to support a legal claim, documentation must include:
- Initial Functional Limitations: Objective measures (cervical range of motion in degrees, pain scale ratings, orthopedic test findings)
- Treatment Rationale: Explanation of why percussor therapy was chosen over alternative interventions
- Progress Tracking: Session-by-session notes documenting objective improvements or lack thereof
- Frequency Justification: Clinical reasoning for treatment frequency and duration
Providers who use advanced diagnostic tools—such as Digital Motion X-Ray (DMX) to visualize ligament instability—create stronger documentation packages because they can correlate soft tissue treatment with structural pathology.
Avoiding “Maintenance Care” Misclassification
Insurance adjusters often challenge soft tissue treatment as “maintenance” or “comfort care” if it extends beyond 12 weeks without documented improvement. To prevent claim denial, treatment plans should establish objective discharge criteria from the outset (e.g., “Continue percussor therapy until cervical rotation improves from 45° to 70° bilaterally, or 12 weeks, whichever occurs first”).
This approach frames percussor therapy as goal-directed rehabilitation rather than open-ended symptom management, aligning with insurance standards for medical necessity.
Patient Safety, Contraindications, and Clinical Standards
While percussor therapy is generally safe for musculoskeletal conditions, certain medical situations require modification or deferral of treatment.
Absolute Contraindications
Percussor therapy should not be used in the following circumstances:
- Active Fractures or Dislocations: Mechanical force could displace bone fragments or worsen joint instability
- Deep Vein Thrombosis (DVT): Percussion over a blood clot could dislodge it, causing pulmonary embolism
- Malignancy in Treatment Area: Direct mechanical stimulation of cancerous tissue is contraindicated
- Acute Infections: Cellulitis, abscess, or osteomyelitis could spread with increased circulation
- Anticoagulant Medications: Warfarin, heparin, or DOACs increase bleeding risk with deep tissue work
Relative Contraindications (Require Modification)
- Pregnancy: Avoid treatment over abdomen and lumbar spine; gentle cervical/upper back work is generally safe
- Recent Surgery (< 8 weeks): Wait for primary wound healing before applying mechanical force to surgical sites
- Osteoporosis: Reduce force and avoid bony prominences to prevent stress fractures
- Neuropathy: Patients with reduced sensation may not be able to report pain, increasing injury risk
Clinical Safety Protocols
Responsible providers follow these standards:
- Pre-Treatment Screening: Review medical history and current medications before initiating percussor therapy
- Informed Consent: Explain the treatment mechanism, expected sensations, and potential adverse effects (temporary soreness, bruising)
- Graduated Force Application: Begin with minimal intensity and increase based on patient tolerance
- Post-Treatment Monitoring: Assess for adverse reactions (increased pain, dizziness, nausea) before discharge
When to Defer Treatment in Favor of Imaging
If a patient presents with “red flag” symptoms—such as bowel/bladder dysfunction, progressive neurological deficits, or fever—advanced imaging (MRI, CT) should be obtained before initiating percussor therapy. The treatment is contraindicated until serious pathology (spinal cord compression, infection, tumor) is ruled out.
This conservative approach protects both patient safety and provider liability, ensuring that mechanical therapy is applied only when appropriate.
Frequently Asked Questions
How does percussor therapy differ from a standard massage gun?
Clinical percussors use perpendicular percussion force at specific therapeutic frequencies (0.5-12 Hz) to penetrate deep fascia and induce mechanotransduction—the cellular process that remodels collagen. Consumer massage guns rely on high-frequency vibration (30-50 Hz) that affects only superficial muscles through a neuromuscular reflex. Clinical devices are also calibrated for medical documentation and require provider training in frequency selection, while consumer devices are general wellness tools without therapeutic specificity.
Is percussor therapy painful for acute injuries?
Percussor therapy is specifically designed for acute injury tolerance. Unlike manual deep tissue work, which requires the practitioner to apply sustained pressure, the percussor delivers intermittent mechanical waves that do not trigger protective muscle guarding. Most patients describe the sensation as “soothing” or “deeply relaxing,” even when treating inflamed tissue. Alpha wave frequencies (8-12 Hz) also activate the parasympathetic nervous system, reducing pain perception during treatment.
Can percussion help with old surgical scar tissue?
Yes, but timing matters. Percussor therapy should not be applied until 8-12 weeks post-surgery, once primary wound healing is complete. After this window, Theta wave frequencies (4-8 Hz) can be used to remodel dense scar tissue by inducing thixotropic changes in the collagen matrix. The piezoelectric effect also stimulates fibroblast activity, encouraging better collagen organization. Treatment is typically performed 1-2 times per week over 8-12 sessions for chronic adhesions.
How long does a typical percussor treatment session last?
A standard clinical session lasts 15-20 minutes of direct percussor application, plus time for assessment and reassessment. The treatment is highly focused—unlike 60-minute massage sessions, percussor therapy targets specific adhesions and restrictions rather than providing full-body relaxation. Sessions are often combined with other modalities (adjustments, decompression, laser) within a 30-45 minute total appointment.
Is there a specific frequency used for fascial release?
Theta wave frequencies (4-8 Hz) are optimal for deep fascial release because they penetrate 3-4 inches into tissue and induce thixotropic changes that temporarily reduce fascial viscosity. This frequency range also stimulates mechanoreceptors that trigger collagen remodeling pathways. For superficial fascial work or lymphatic drainage, Delta waves (0.5-4 Hz) are used. Alpha waves (8-12 Hz) are reserved for nervous system modulation rather than structural release.
Can percussor therapy trigger an emotional release?
Yes, this phenomenon is recognized in bodywork literature as “somato-emotional release.” Fascia stores mechanical tension patterns related to trauma, and when chronic restrictions are released, some patients experience spontaneous emotional responses (crying, laughter, anger). This is particularly common when treating the diaphragm, psoas muscle, or suboccipital region—areas with high vagus nerve density. Providers trained in trauma-informed care recognize this as a normal response and provide appropriate support.
How soon can I exercise after a percussor treatment?
For gentle activity (walking, light stretching), there are no restrictions—patients can resume immediately. For moderate to intense exercise (running, weightlifting, contact sports), wait 24-48 hours to allow the tissue remodeling process to stabilize. The thixotropic changes induced by percussion make fascia temporarily more pliable, which is beneficial for movement but could increase injury risk if loaded aggressively too soon. Your provider will give specific guidance based on injury severity.
Does insurance cover percussor therapy in Colorado?
Yes, when billed as therapeutic soft tissue mobilization under an active auto injury claim or Med-Pay policy. Colorado Med-Pay typically covers 100% of medically necessary treatment up to policy limits ($5,000-$100,000). Percussor therapy must be part of a documented treatment plan with objective goals and progress tracking. For non-accident cases, coverage depends on your health insurance policy—many plans cover it as part of chiropractic or physical therapy benefits, but pre-authorization may be required.
What conditions respond best to percussor therapy?
The strongest outcomes are seen in: (1) Acute whiplash and cervical strain (0-6 months post-injury), where muscle guarding prevents manual therapy tolerance; (2) Chronic adhesions from old injuries or surgery that limit range of motion; (3) Lymphatic congestion and edema from seatbelt injuries or surgical disruption; (4) Plantar fasciitis, IT band syndrome, and other dense fascial restrictions; (5) Tension-type headaches related to suboccipital muscle tightness. Conditions with nerve damage or bone pathology (fractures, arthritis) respond less predictably.
How many sessions are typically needed to see results?
Acute injuries often show measurable improvement in range of motion or pain within 3-5 sessions (1-2 weeks of treatment). Chronic adhesions or scar tissue may require 8-12 sessions over 4-6 weeks before significant functional changes occur. The key variable is tissue quality—well-vascularized tissue remodels faster than dense, fibrotic tissue. Providers should document objective progress (e.g., “Cervical rotation improved from 45° to 60° after 4 sessions”) to justify continued treatment.
Can percussor therapy be used on the same day as chiropractic adjustments?
Yes, and this is one of the most effective combinations. Percussor therapy is typically performed before adjustments to release muscle guarding and fascial restrictions that resist joint mobilization. This allows the adjustment to be more specific and less forceful, improving patient comfort and outcomes. Some providers also apply gentle percussion after adjustments to reduce post-manipulation soreness. The two modalities address different tissue layers (fascia vs. joint capsule) and complement each other well.
Is percussor therapy the same as instrument-assisted soft tissue mobilization (IASTM)?
No. IASTM (such as Graston Technique) uses rigid metal tools to scrape along tissue with manual force, creating controlled microtrauma that stimulates inflammation and remodeling. Percussor therapy uses motorized percussion that delivers frequency-specific mechanical waves without surface friction or scraping. IASTM is more aggressive and often causes bruising; percussor therapy is gentler and suitable for acute injury phases. Both fall under the broader category of mechanical soft tissue mobilization, but the mechanisms and applications differ significantly.