
Sciatica Pain Relief
Sciatica Pain Relief: Complete Guide to Causes, Diagnosis & Non-Surgical Treatment
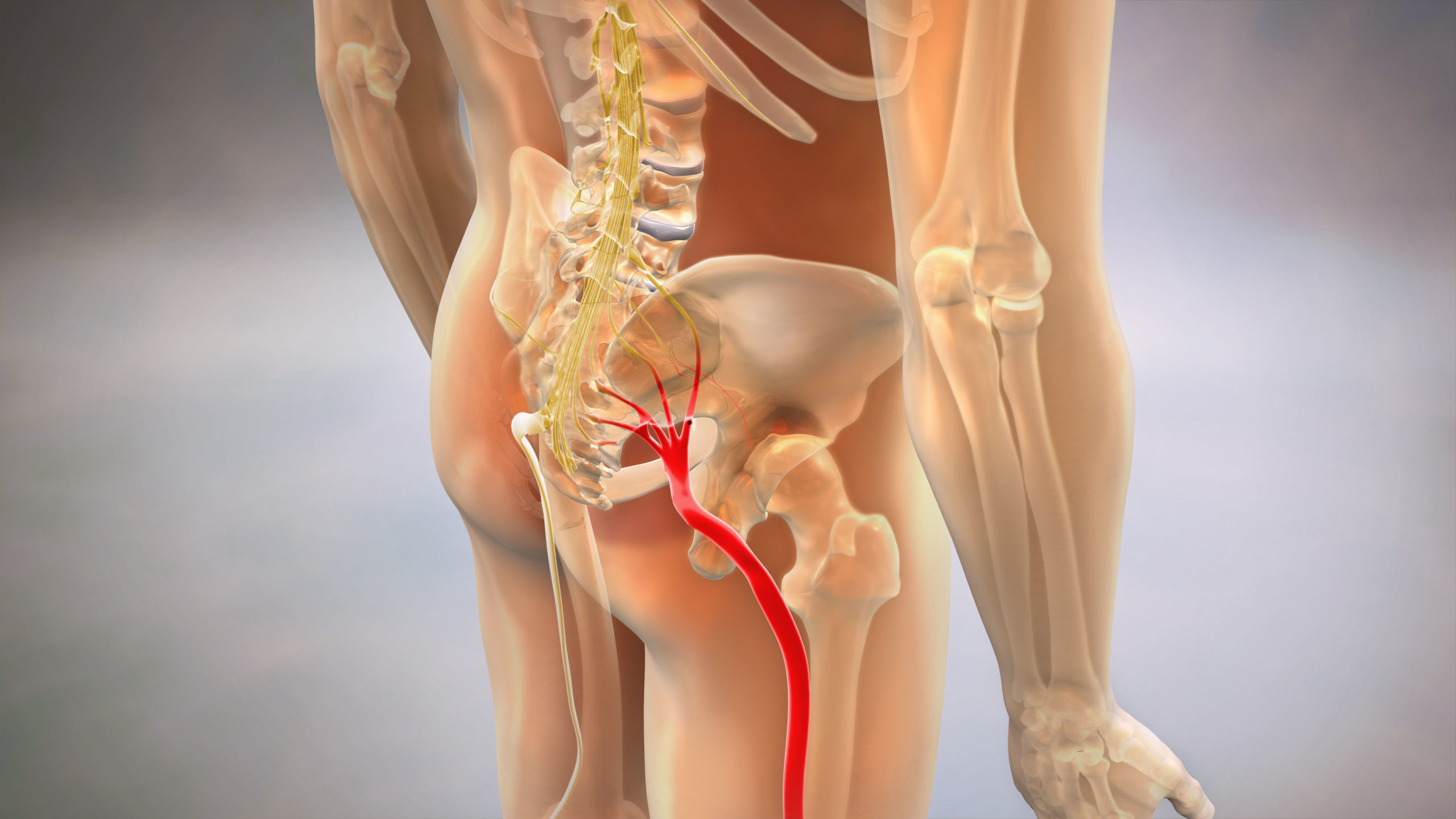
Sciatica, medically known as lumbar radiculopathy, refers to pain that radiates along the path of the sciatic nerve—from the lower back through the hips, buttocks, and down each leg. While often caused by degenerative disc disease, sciatica can also result from acute trauma such as auto accidents, creating distinct diagnostic and treatment considerations. The sciatic nerve is the longest and widest nerve in the human body, and when compressed or irritated, it can produce symptoms ranging from mild tingling to debilitating pain that affects mobility and quality of life.
Table of Contents[Hide][Show]
Need Specialized Treatment for Your Sciatica?
If you’re experiencing sciatic nerve pain following an auto accident or need advanced non-surgical care, our Colorado providers offer targeted treatment protocols:

Complete Car Accident Treatment Protocol – Comprehensive care for crash-related injuries

Non-Surgical Spinal Decompression Therapy – Relief for disc herniation and nerve compression

Therapeutic Laser Treatment – Advanced pain management and tissue healing

Chiropractic Adjustments for Sciatica – Targeted spinal corrections

Percussor Therapy – Deep tissue treatment for muscle tension
Find a Traumatic Injury Specialist Near You
What Causes Sciatica? The Nerve Pathway Explained
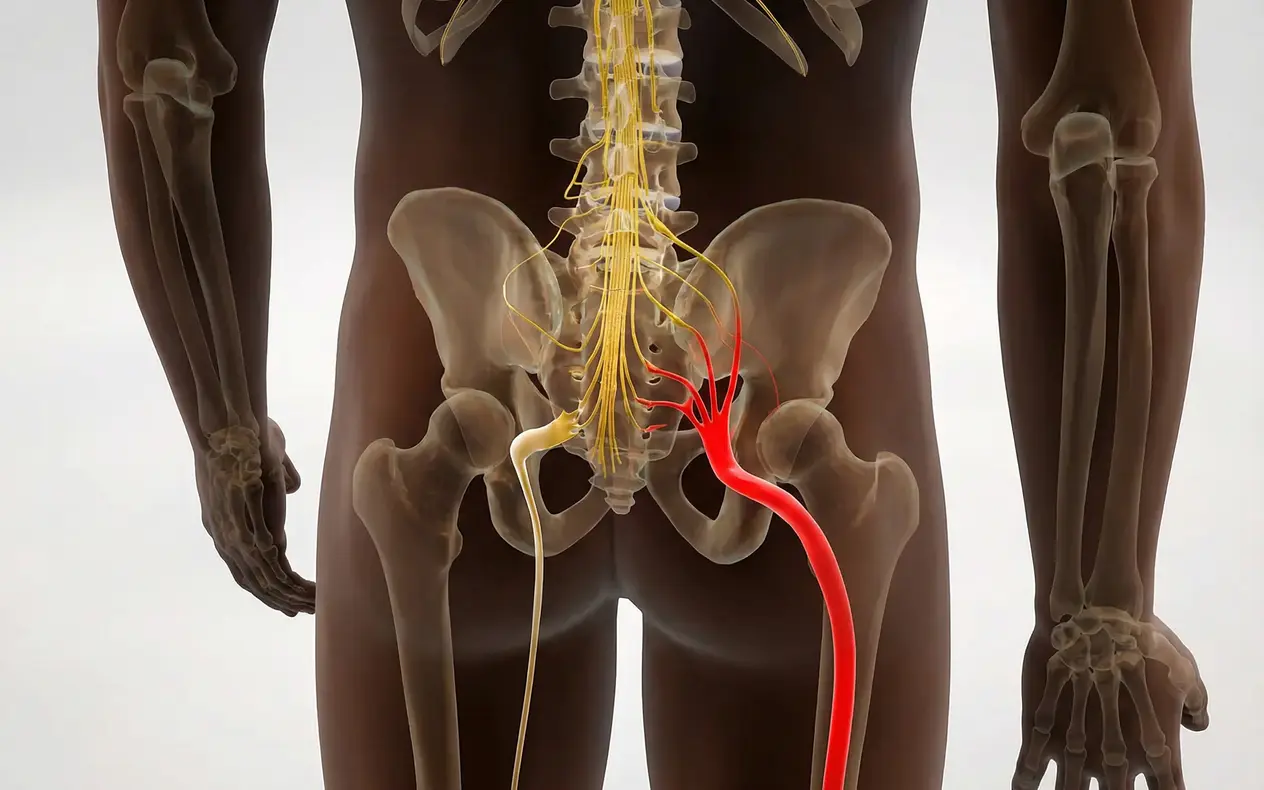
The sciatic nerve originates from five nerve roots in the lower lumbar and sacral spine—specifically the L4, L5, S1, S2, and S3 vertebral levels. These nerve roots exit the spinal column through small openings called foramina and converge to form the thick sciatic nerve that travels down each leg. Understanding this pathway is essential because the location and pattern of your pain can indicate which specific nerve root is being compressed.
When the sciatic nerve or its contributing nerve roots become compressed, inflamed, or irritated, pain signals travel along predictable pathways called dermatomes. For example, compression at the L5 nerve root typically causes pain or numbness along the outer calf and top of the foot, while S1 nerve root compression affects the back of the leg and outer edge of the foot. This specificity is why an experienced provider can often identify the exact source of compression based on your symptom distribution alone.
Several structures can cause sciatic nerve compression. The most common culprit is a herniated or bulging disc—the gel-like cushions between vertebrae that can rupture or protrude outward, pressing directly on nerve roots. Other causes include spinal stenosis (narrowing of the spinal canal), spondylolisthesis (vertebral slippage), bone spurs from degenerative arthritis, or in rare cases, tumors or infections. Muscle-based compression, particularly from the piriformis muscle in the buttock, can mimic sciatica but involves a different mechanism.
The reason your leg hurts even though the problem is in your back comes down to referred pain—the nervous system’s way of mapping internal injury to surface sensations. The nerve compression happens in the spine, but your brain interprets the pain as coming from the areas that nerve supplies. This is why treating only the leg symptoms without addressing the spinal source rarely provides lasting relief.
Traumatic Sciatica vs. Degenerative Sciatica: Critical Differences
While sciatica symptoms may appear similar regardless of cause, the distinction between traumatic and degenerative sciatica has profound implications for diagnosis, treatment, and legal documentation. Understanding this difference is particularly crucial for Colorado residents who develop sciatica following an auto accident.
Degenerative sciatica develops gradually over months or years due to age-related wear and tear on spinal structures. The discs naturally lose water content and height with aging, causing them to bulge or herniate slowly. Facet joints develop arthritis, bone spurs form, and the spinal canal narrows incrementally. Patients often describe a history of intermittent back pain that gradually worsened, with leg symptoms appearing only in later stages. This process is considered a natural consequence of aging and is rarely associated with a single causative event.
Traumatic sciatica, by contrast, occurs suddenly following a specific injury mechanism—most commonly rear-end or side-impact collisions. The biomechanical forces involved in motor vehicle accidents (MVA) create what researchers call cervical and lumbar acceleration-deceleration injuries. During impact, the torso is restrained by the seatbelt while the head and lower spine experience rapid forward-and-backward or rotational movement. This creates shearing forces on the intervertebral discs, often causing acute herniation or extrusion of disc material into the spinal canal.
Equally important but often missed is the concept of ligament laxity. The ligaments that normally stabilize spinal segments can be stretched or torn during the accident, creating abnormal movement patterns that don’t appear on standard static imaging. This hidden instability can cause intermittent nerve compression that varies with position—something that requires specialized diagnostic approaches to detect.
The timeline is a key differentiator. While degenerative sciatica often has a vague onset (“it’s been bothering me for years”), traumatic sciatica typically begins within hours to days of the accident. Patients frequently report that they initially felt only minor soreness, but within 24-72 hours, severe radiating leg pain developed. This delayed onset is characteristic of post-traumatic disc herniation, as the inflammatory cascade takes time to fully develop.
From a medical-legal standpoint, this distinction is critical. Insurance companies and their computerized claims evaluation software (such as Colossus) are programmed to minimize payouts for “pre-existing degenerative conditions.” If your MRI shows any age-related changes—which virtually all adults over 30 have—adjusters will argue your sciatica was not caused by the accident. This is where proper documentation of the traumatic mechanism, the acute timeline, and the use of specialized diagnostic tools like Digital Motion X-Ray becomes essential to prove causation.
Colorado Med-Pay insurance policies (mandated under C.R.S. § 10-4-635) are designed to cover medically necessary treatment for accident-related injuries without regard to fault. However, establishing that your sciatica is accident-related rather than pre-existing requires clinical documentation that connects the trauma mechanism to your current symptoms. This is not the kind of documentation provided by a quick 10-minute adjustment at a strip-mall chiropractic clinic.
Diagnostic Protocols: Beyond the Standard MRI
Most patients with sciatica are sent for a standard MRI scan, which provides detailed images of disc herniations, nerve root compression, and spinal cord integrity. MRI is the gold standard for visualizing soft tissue pathology and is essential for ruling out serious conditions like tumors or infections. However, MRI has a significant limitation: it is a static imaging study taken while you lie perfectly still in a tube.
The problem with static imaging is that it cannot capture dynamic instability—the abnormal movement between vertebrae that occurs during normal motion. If your ligaments were injured during the accident, your spine may shift abnormally when you bend, twist, or bear weight, but this instability disappears when you lie flat for the MRI. The result is that the MRI may appear “normal” or show only “mild degenerative changes,” even though you experience severe pain during daily activities.
This is where Digital Motion X-Ray (DMX) provides diagnostic value that traditional imaging cannot. DMX captures fluoroscopic video (essentially a real-time X-ray movie) while you actively flex, extend, and rotate your spine. It reveals abnormal translation (sliding), excessive rotation, or instability at specific spinal segments that would be invisible on static MRI. For traumatic injury cases, DMX can demonstrate ligament damage that explains persistent pain despite “normal” MRI findings.
The clinical protocol for comprehensive sciatica diagnosis should include:
Phase 1: Clinical Examination
- Straight leg raise test (Lasègue’s sign)
- Neurological assessment (reflexes, sensation mapping, motor strength)
- Dermatome pattern mapping to isolate the specific nerve root
- Orthopedic provocative tests to differentiate spinal vs. peripheral causes
Phase 2: Static Imaging
- MRI of the lumbar spine to identify disc herniations, stenosis, or space-occupying lesions
- Standing lumbar X-rays to assess alignment, spondylolisthesis, and overall spinal architecture
Phase 3: Dynamic Imaging (for trauma cases)
- Digital Motion X-Ray to document ligament laxity and segmental instability
- Comparison to normative data to quantify excessive motion
Phase 4: Electrodiagnostic Studies (when indicated)
- EMG/NCV (electromyography/nerve conduction velocity) to confirm nerve damage and rule out peripheral neuropathy
- Typically reserved for cases with progressive weakness or surgical consideration
For Colorado patients involved in auto accidents, the combination of MRI and DMX creates a comprehensive diagnostic record that not only guides treatment but also provides the objective documentation required for insurance claims and potential litigation. The AMA Guides to the Evaluation of Permanent Impairment (5th and 6th editions), which are the standard reference for injury severity ratings used in legal settlements, specifically recognize the value of documenting both structural pathology (MRI) and functional instability (dynamic imaging).
Non-Surgical Treatment Options for Sciatica Relief

The majority of sciatica cases—even those involving significant disc herniations—can be successfully managed without surgery using evidence-based conservative care protocols. The key is implementing a staged treatment approach that addresses the three distinct phases of healing: acute pain control, structural correction, and functional restoration.
Phase 1: Neuro-Desensitization (Acute Pain Management)
When you’re in the acute phase of sciatica, the nervous system is in a hypersensitive state. The inflamed nerve roots send constant pain signals, and even minor movements can trigger muscle spasms. The goal of Phase 1 is not to “fix” the underlying problem immediately, but to calm the nervous system enough to allow healing to begin.
Therapeutic modalities used in this phase include:
Low-Level Laser Therapy (LLLT) uses specific wavelengths of light to reduce inflammation at the cellular level. Unlike heat or ice, which only affect surface tissues, therapeutic lasers penetrate deep into the disc space and nerve roots to accelerate healing and reduce the inflammatory cascade that perpetuates pain.
Percussor Therapy provides rapid, controlled mechanical vibration to reduce muscle guarding and spasm in the paraspinal muscles. When your sciatic nerve is inflamed, the surrounding muscles often lock up as a protective response, but this muscle tension actually worsens nerve compression. Percussor therapy breaks this cycle.
Gentle spinal mobilization (not high-velocity manipulation in the acute phase) can restore basic movement patterns without aggravating the inflamed nerve. The goal is to prevent the development of compensatory movement patterns that create secondary problems.
Phase 2: Spinal Decompression (Structural Correction)
Once the acute pain begins to subside, Phase 2 addresses the underlying structural problem: the compressed nerve root. Non-Surgical Spinal Decompression is the cornerstone of this phase.
Spinal decompression uses computer-controlled traction to create negative pressure within the disc space. This negative pressure serves two purposes: it can draw herniated disc material back toward the center (the nucleus pulposus), and it promotes the influx of nutrients and oxygen into the damaged disc, facilitating healing. Unlike old-style traction tables that simply stretched the spine, modern decompression systems use intermittent cycles of distraction and relaxation to avoid triggering muscle guarding.
The typical decompression protocol involves 20-30 sessions over 6-8 weeks, with each session lasting 20-30 minutes. Research published in the Journal of Neurological Research has demonstrated that properly administered spinal decompression can result in a 70-80% reduction in radiating pain for patients with confirmed disc herniations, without the risks associated with surgery.
This phase may also include targeted chiropractic adjustments to address joint fixations that develop as the body compensates for sciatic pain. When you favor one leg or shift your weight to avoid pain, you create abnormal stress on other spinal segments, which can lead to secondary restrictions that perpetuate symptoms even after the disc heals.
Phase 3: Biomechanical Stabilization (Functional Restoration)
The final phase focuses on preventing recurrence by addressing the biomechanical dysfunction that made your spine vulnerable to injury in the first place. This is where most “generic” chiropractic care fails—it stops once the pain is gone, leaving the underlying weakness unaddressed.
Core stabilization exercises strengthen the deep spinal muscles (multifidus, transverse abdominis) that maintain proper spinal alignment during movement. Research consistently shows that core weakness is a primary risk factor for both initial disc herniation and recurrent episodes.
McKenzie Method protocols teach you specific directional exercises based on your symptom response. Some patients experience centralization (reduction of leg pain) with extension exercises, while others respond to flexion-based movements. The McKenzie approach creates a personalized exercise prescription based on your unique pain pattern.
Ergonomic and activity modification training addresses the lifestyle factors that contribute to sciatica. For auto accident victims returning to work, this might include proper lifting mechanics, seated posture optimization, or modifications to prevent prolonged static positioning that increases disc pressure.
The goal of Phase 3 is to transition you from passive treatment (where things are done to you) to active self-management (where you have the tools to maintain your recovery long-term). Patients who complete all three phases have significantly lower recurrence rates than those who stop treatment once symptoms improve.
Medical-Legal Documentation for Accident-Related Sciatica
If your sciatica developed following a motor vehicle accident, the quality of your medical documentation will directly impact your ability to obtain fair compensation from insurance carriers. This section addresses the critical gap between basic chiropractic notes and the comprehensive medical-legal documentation required for injury claims.
Why Generic Notes Fail in Insurance Claims
Most chiropractic clinics—particularly high-volume “adjustment mills”—use templated documentation that simply records the date, the technique used, and a brief subjective complaint. A typical note might read: “Patient reports lower back and leg pain. Adjustment performed to L5-S1. Patient tolerated treatment well.” While this satisfies basic compliance requirements, it provides zero value in an insurance or legal context.
Insurance adjusters and their computerized claims software (such as Colossos or Claimant IQ) are programmed to minimize payouts by exploiting gaps in documentation. If your treatment records don’t explicitly connect your symptoms to the accident mechanism, don’t document objective findings, and don’t reference medical-legal standards, the insurer will argue that your treatment was not medically necessary, not causally related to the accident, or excessive compared to “standard care.”
The Components of AMA-Compliant Documentation
The AMA Guides to the Evaluation of Permanent Impairment (5th and 6th editions) provide the standardized methodology for assessing injury severity and permanent impairment in medico-legal contexts. Any provider who treats traumatic injury cases must document using this framework.
Causation Analysis: The initial evaluation must include a detailed narrative that explains the biomechanical mechanism of your injury. For sciatica following a rear-end collision, this includes documenting the direction of impact, estimated force (based on vehicle damage), position of your body at the time of impact, and the specific mechanism by which acceleration-deceleration forces could have caused acute disc herniation or ligament injury. This is not speculation—it’s applied biomechanics.
Objective Findings: Every treatment note should include measurable, reproducible findings. This includes specific neurological deficits (decreased reflexes, dermatomal sensory loss, motor weakness measured by manual muscle testing), positive orthopedic tests (straight leg raise angle in degrees), and range of motion measurements using inclinometry. These objective markers demonstrate that your complaints are not subjective exaggeration but have verifiable clinical correlates.
Diagnostic Imaging Correlation: The documentation must reference your MRI and DMX findings and explain how the imaging abnormalities correlate with your clinical presentation. For example: “Patient’s left lateral leg pain and foot numbness correspond to L5 dermatome, consistent with MRI findings of left lateral disc herniation at L5-S1 with compression of the traversing L5 nerve root.” This correlation proves that your symptoms have an anatomical basis.
Treatment Rationale: Each treatment session should include a brief rationale explaining why that specific intervention is medically necessary. For spinal decompression, this might state: “Continued decompression therapy indicated to reduce intradiscal pressure and promote retraction of herniated nucleus pulposus, as conservative management of documented L5-S1 disc herniation.” This language demonstrates that treatment decisions are based on clinical reasoning, not arbitrary protocols.
Functional Capacity Documentation: The records should document how your injury impacts daily activities using standardized scales or narrative descriptions. This might include inability to sit for more than 20 minutes without increased leg pain, difficulty with prolonged standing, limitation in lifting capacity, or disruption of sleep due to positional pain. These functional limitations translate directly into “pain and suffering” calculations in settlements.
Impairment Rating (when appropriate): If you reach maximum medical improvement with residual symptoms, a formal impairment rating using the AMA Guides methodology provides an objective measure of permanent injury. Even a 5% whole person impairment can represent tens of thousands of dollars in settlement value.
Colorado Med-Pay and Your Rights
Colorado law requires all auto insurance policies to include Medical Payments (Med-Pay) coverage of at least $5,000 (C.R.S. § 10-4-635), though many policies carry higher limits. Med-Pay is first-party coverage, meaning it pays for your medical expenses regardless of who was at fault in the accident, and it’s available immediately—no waiting for the liability claim to settle.
Crucially, Colorado Med-Pay covers chiropractic care when it is medically necessary for treatment of accident-related injuries. However, insurance companies will often claim that treatment has become “maintenance care” or is not causally related to the accident if documentation is inadequate. This is why the medical-legal narrative is essential from day one.
If you are represented by a personal injury attorney, your chiropractor should be prepared to communicate directly with your legal team and provide narrative reports, records, and potentially expert testimony if the case proceeds to litigation. Providers who specialize in traumatic injury understand this requirement; general wellness chiropractors typically do not.
The financial implications are significant. According to the Colossus algorithm used by many insurers, the same sciatica injury might generate a $15,000 settlement if documented with generic notes, but a $45,000+ settlement if supported by AMA-compliant medical-legal documentation. The injury is identical—the documentation makes the difference.
When to Seek Immediate Care: Red Flag Symptoms

While most sciatica cases are painful but not medically dangerous, certain “red flag” symptoms indicate potential emergencies that require immediate medical evaluation. These symptoms suggest possible cauda equina syndrome—a rare but serious condition where severe compression affects multiple nerve roots simultaneously.
Seek emergency care immediately if you experience:
Saddle anesthesia: Numbness in the groin, inner thighs, or around the rectum. This indicates compression of the sacral nerve roots that control bowel and bladder function.
Bowel or bladder dysfunction: New inability to control urination or defecation, or conversely, inability to urinate (urinary retention). Cauda equina syndrome can cause permanent nerve damage if not surgically decompressed within 24-48 hours.
Bilateral leg symptoms: While sciatica typically affects one leg, sudden pain or numbness in both legs simultaneously may indicate severe central disc herniation compressing multiple nerve roots.
Progressive weakness: If your foot drop (inability to lift your foot) or leg weakness is worsening rapidly over hours to days, this suggests ongoing nerve damage that may require urgent intervention.
Fever with back pain: The combination of severe back pain and fever may indicate spinal infection (discitis or epidural abscess), which is a medical emergency.
Other concerning symptoms that warrant prompt (though not necessarily emergency) evaluation include severe pain that doesn’t improve at all with position changes, night pain that wakes you from sleep and is unrelieved by any position, or history of cancer with new onset back/leg pain (possible metastatic disease).
For the vast majority of patients, sciatica—while severely painful—is not dangerous and will improve with appropriate conservative care. However, monitoring for these red flags ensures that serious complications are not missed.
Frequently Asked Questions About Sciatica
How long does a typical sciatica flare-up last without surgery?
The natural history of sciatica varies significantly based on the underlying cause and severity. For acute traumatic sciatica (such as from an auto accident), most patients experience substantial improvement within 6-12 weeks with appropriate conservative care. Research shows that approximately 60-70% of patients achieve significant pain relief within 12 weeks using non-surgical treatment protocols.
However, “improvement” doesn’t always mean complete resolution. Many patients transition from severe constant pain to occasional flare-ups triggered by specific activities. Without proper rehabilitation and biomechanical correction, recurrence rates can exceed 40% within the first year. This is why completing all three phases of treatment—acute care, structural correction, and functional restoration—is critical for long-term outcomes.
For degenerative sciatica, the timeline is often more prolonged and may involve periods of remission and exacerbation over months to years. The key factor is whether the underlying cause (such as a disc herniation) is capable of healing. Some disc herniations partially reabsorb over time as the body’s immune system breaks down the herniated material, while others persist indefinitely.
What is the difference between sciatica and piriformis syndrome?
While both conditions cause buttock and leg pain, the underlying mechanisms differ significantly. True sciatica results from nerve root compression at the spinal level—typically from a herniated disc, spinal stenosis, or spondylolisthesis. The compression occurs where the nerve roots exit the spine, and symptoms follow the specific dermatome pattern associated with the affected nerve root.
Piriformis syndrome occurs when the piriformis muscle (a small muscle deep in the buttock) becomes tight or spasms and compresses the sciatic nerve as it passes through or beneath the muscle. This is considered a “peripheral” nerve entrapment rather than a spinal problem. Symptoms can mimic sciatica but often have slightly different characteristics—the pain is typically more localized to the buttock, may be aggravated by hip rotation or prolonged sitting, and doesn’t always follow classic dermatomal patterns.
Diagnostic examination can usually differentiate the two. The FAIR test (Flexion, Adduction, Internal Rotation) is specific for piriformis syndrome, while a positive straight leg raise test suggests spinal nerve root involvement. MRI will show disc herniation in true sciatica but typically appears normal in isolated piriformis syndrome. In practice, many patients have elements of both—the spinal nerve root is irritated, which causes secondary muscle spasm including the piriformis, creating a compound problem.
Is walking good for sciatica or does it aggravate the nerve?
The answer depends on the specific mechanism and severity of your sciatica. For most patients with mild to moderate symptoms, walking is beneficial because it promotes circulation, maintains range of motion, and prevents the deconditioning that occurs with prolonged bed rest. Studies consistently show that complete bed rest for more than 2-3 days actually delays recovery and can worsen outcomes.
However, the key is moderation and monitoring your symptom response. If walking causes your leg pain to move further down the leg (peripheralization), this is generally a negative sign indicating increased nerve irritation. Conversely, if walking causes your pain to retreat back toward the spine (centralization), this is a positive sign suggesting the activity is beneficial. The McKenzie Method uses this principle to guide activity recommendations.
For severe acute sciatica—particularly in the first few days after injury when inflammation is at its peak—even minimal walking may be intolerable. In this phase, short periods of gentle movement alternating with rest is appropriate. As inflammation subsides, gradually increasing walking distance and frequency promotes healing.
Pay attention to your walking mechanics. If you’re limping significantly or hiking your hip to avoid leg pain, the compensatory movement patterns may create secondary problems in other areas. Using a temporarily assistive device (cane) or reducing distance may be appropriate until your gait normalizes.
What constitutes “red flag” symptoms for sciatica requiring emergency care?
While covered in detail earlier, the critical red flags warrant repeating because missing these symptoms can lead to permanent neurological damage. Seek immediate emergency evaluation if you develop:
- Loss of bowel or bladder control (incontinence or retention)
- Saddle anesthesia (numbness in the groin or rectal area)
- Progressive motor weakness (foot drop that’s worsening over hours to days)
- Bilateral leg symptoms (both legs affected simultaneously)
- Fever with back pain (possible spinal infection)
These symptoms may indicate cauda equina syndrome or spinal infection, both of which require emergency surgical intervention. The window for preventing permanent damage is narrow—typically 24-48 hours from symptom onset. Do not “wait and see” if you develop these symptoms.
Can sciatica cause permanent nerve damage if left untreated?
In most cases, sciatica does not cause permanent damage even if left untreated, because the body’s natural healing mechanisms will eventually reduce inflammation and swelling around the nerve root. Many disc herniations partially reabsorb over time through a process called phagocytosis, where immune cells gradually break down the herniated disc material.
However, there are important exceptions. If nerve compression is severe and prolonged, it can cause axonal damage (injury to the nerve fibers themselves) rather than just temporary irritation. This is more likely when there is significant structural compression visible on MRI—such as a large extruded disc fragment or severe spinal stenosis—combined with objective neurological deficits like muscle weakness or loss of reflexes.
The concept of the “therapeutic window” is important here. Early intervention, particularly within the first 6-12 weeks, has the best chance of preventing progression to permanent injury. Once nerve fibers die (which shows up on EMG as fibrillation potentials), recovery becomes much more limited. The nerve may partially regenerate, but this process is slow (approximately 1mm per day) and often incomplete.
This is why objective neurological monitoring is essential. If you have measurable weakness (inability to stand on toes or heels), absent reflexes, or significant sensory loss, more aggressive intervention—whether advanced conservative care or surgical consultation—should be pursued rather than adopting a “wait and see” approach.
What are the best sleeping positions to relieve sciatic nerve pressure?
Sleep position can significantly impact sciatic pain by either relieving or increasing pressure on the affected nerve root. The optimal position depends on your specific pain pattern, but general principles apply.
For most people with sciatica, sleeping on the side with a pillow between the knees is most comfortable. This position maintains neutral spine alignment and prevents the top leg from rotating the pelvis forward, which can increase tension on the sciatic nerve. The pillow should be thick enough to keep your hips level rather than allowing the top leg to drop downward.
Back sleeping can work well if you place a pillow under your knees to maintain the natural lumbar curve. This position reduces pressure on the lumbar discs and keeps the spine in neutral alignment. Some patients find that elevating the legs higher (on two pillows or a wedge) further reduces nerve tension.
Stomach sleeping is generally the worst position for sciatica because it forces excessive lumbar extension and often requires rotating your head to the side, creating rotational stress on the spine. If you’re a committed stomach sleeper, placing a pillow under your hips can reduce lumbar hyperextension.
Mattress firmness matters more than sleeping position for some patients. A mattress that’s too soft allows the pelvis to sink while the shoulders remain elevated, creating lateral curvature. Conversely, an excessively firm mattress may create pressure points that prevent comfortable positioning. Medium-firm is generally optimal for most people with sciatica.
How does hydration affect spinal disc health and nerve pain?
Intervertebral discs are approximately 80% water in young, healthy individuals, though this percentage decreases with age. The disc has no direct blood supply, so it relies on a process called imbibition—the passive diffusion of nutrients and water from surrounding tissues. Adequate hydration is essential for maintaining disc height and resilience.
When you’re dehydrated, disc height can decrease measurably within hours. This reduction in disc height has two negative effects: it reduces the size of the foraminal openings where nerve roots exit (increasing potential for compression), and it reduces the disc’s shock-absorbing capacity, making it more vulnerable to injury under loading.
Research has shown that people who are chronically dehydrated have higher rates of disc degeneration and herniation. While drinking water won’t reverse an existing disc herniation, maintaining proper hydration can help optimize the disc’s healing capacity and reduce the risk of recurrence.
The practical recommendation is to consume half your body weight in ounces of water daily. So if you weigh 160 pounds, aim for 80 ounces (about 2.5 liters) of water throughout the day. This is particularly important for patients undergoing spinal decompression therapy, as the negative pressure created during treatment is most effective when the disc is well-hydrated and capable of absorbing nutrients.
Caffeine and alcohol have mild diuretic effects, so if you consume these regularly, slightly increase your water intake to compensate. The color of your urine is a simple indicator—pale yellow indicates adequate hydration, while dark yellow suggests you need more fluids.